Browse our range of reports and publications including performance and financial statement audit reports, assurance review reports, information reports and annual reports.
Auditor-General Report No. 48 of 2012–13
Management of the Targeted Community Care (Mental Health) Program
Published
Wednesday 19 June 2013
Portfolio
Families, Housing, Community Services & Indigenous Affairs
Entity
Department of Families, Housing, Community Services and Indigenous Affairs
Contact
Please direct enquiries relating to reports through our contact page.
Sector
Social Services
The objective of the audit was to assess the effectiveness of the Department of Families, Housing, Community Services and Indigenous Affairs' (FaHCSIA) administration and management of the Targeted Community Care (Mental Health) Program.
Summary
Introduction
1. Mental illness is a significant health issue in Australia affecting the lives of individuals, their carers and the wider community1. Awareness of the scale of mental illness, and its extensive social impact, has increased substantially over the past decade, both by governments and the general population.2 The Department of Families, Housing, Community Services and Indigenous Affairs (FaHCSIA) has estimated the annual cost of productivity losses attributable to mental illness to range from $10 billion to $15 billion.3
2. Almost half the Australian population aged 16 to 85 years has experienced a mental illness episode at some point in their life4 and for most people who experience mental illness in adult life, the illness has its onset in childhood or adolescence.5 In 2006, following two reports6 highlighting the need for services to assist people with mental illness and to increase coordination between clinical and community-based services, the Council of Australian Governments (COAG) agreed on a whole-of-government approach to mental health. This was implemented through the National Action Plan on Mental Health 2006–11 (Action Plan).
3. The four key outcomes of the Action Plan were to:
- reduce the prevalence and severity of mental illness in Australia;
- reduce the prevalence of risk factors that contribute to the onset of mental illness and prevent longer term recovery;
- increase the proportion of people with an emerging or established mental illness who are able to access the right health care and other relevant community services at the right time, with a particular focus on early intervention; and
- increase the ability of people with a mental illness to participate in the community, employment, education and training, including through an increase in access to stable accommodation.7
4. Supporting this agreement, in 2006–07 the Australian Government committed a total of $1.8 billion for 19 initiatives to assist people with mental illness, their families and carers over the five year period 2006–07 to 2010–11. Within this funding, FaHCSIA was allocated $554.7 million for the Targeted Community Care (Mental Health) Program (TCC). The program was directed at the Action Plan’s primary aim of improving mental health and the recovery from illness through a greater focus on promotion, prevention, early intervention and access to mental health services.8
5. The Australian Government committed an additional $2.2 billion for National Mental Health Reforms in May 2011. As part of the Government’s additional funding, $269.3 million was allocated to FaHCSIA over five years to provide further support to community mental health by expanding the TCC Program to include additional service types and locations.
Targeted Community Care (Mental Health) Program
6. The objective of the TCC Program ‘... is to implement community mental health initiatives to assist people with mental illness and their families and carers to manage the impact of mental illness.’9 FaHCSIA’s strategy to achieve the objective is to provide accessible, responsive, high quality and integrated community-based mental health services that improve the capacity of individuals, families and carers to manage the impacts of mental illness on their lives and improve their overall wellbeing.10 FaHCSIA considers that progress towards this outcome will be demonstrated by the social and economic participation of people with a mental illness, together with their carers and families.
7. There are three components to the TCC Program:
- Personal Helpers and Mentors (PHaMs). This initiative is designed to assist people whose lives are severely affected by mental illness by providing support: to manage daily activities; gain access to needed services such as accommodation, social support, health, welfare, and employment services; and increase connections with their community;
- Family Mental Health Support Services11 (FMHSS). This initiative provides early intervention support to assist vulnerable families with children and young people who are at risk of, or affected by, mental illness. These services aim to support parents to reduce family stress and enable children and young people to reach their potential; and
- Mental Health Respite: Carer Support12 (MHR: CS). This initiative funds 650 respite care places which provide a range of flexible respite and support options for carers and families of people with severe mental illness and carers of people with an intellectual disability.
8. The TCC Program complements clinical health services by providing support options that seek to promote social inclusion and recovery. Grant funding is awarded under the TCC Program to community-based not-for-profit organisations and established national charitable organisations to deliver services in sites across Australia. Table S1 shows the number of service sites funded in 2011–12, the number of clients FaHCSIA estimates it has assisted and the funding allocation by each service type.
Table S.1 Targeted Community Care (Mental Health) Program 2011–12
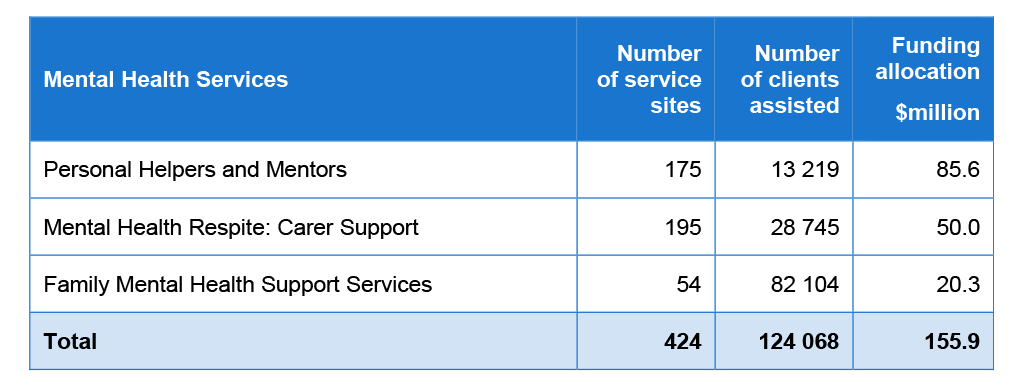
Source: FaHCSIA.
Notes: Number of clients assisted includes remote participants.
Number of service sites is as at 30 June 2012.
Of the 175 PHaMs sites, 95 were in metropolitan areas, 69 were in non-metropolitan areas and 11 were in remote areas.
9. FaHCSIA is currently implementing the expansion of the TCC Program in a staged manner. The department completed four grant selection processes in 2012 – two PHaMs rounds and one each of FMHSS and MHR: CS – and finalised two further FMHSS and MHR: CS rounds in April 2013.
Audit objective, scope and criteria
10. The objective of the audit was to assess the effectiveness of FaHCSIA’s administration and management of the Targeted Community Care (Mental Health) Program.
11. The audit focused primarily on the program’s administration and management since 2010–11. This period included the:
- finalisation of the original program measures; and
- commencement of program expansion measures.
12. Three high level criteria were used to conclude against the audit objective. These were whether FaHCSIA:
- established and used structured and appropriate planning processes to support the targeting of the program;
- managed the selection of service providers consistently with Australian Government requirements; and
- developed and implemented satisfactory performance reporting arrangements for program effectiveness and accountability.
Overall conclusion
13. The Targeted Community Care (Mental Health) Program (TCC) is a series of community-based services designed to support people with a mental illness, and their families and carers. The TCC Program was developed to complement the provision of clinical-based mental health services and, accordingly, to increase access to a range of mental health services. Since 2006–07, the Australian Government has committed over $800 million to services provided through the TCC Program. With this funding, services have been established in 424 locations across Australia, leading to greater access to community-based mental health services. Further expansion is underway which will lead to the establishment of additional service models and locations and increased access to services.
14. Overall, FaHCSIA’s administration of the TCC Program has been generally effective. In determining site locations for the initial program and for the subsequent expansion, the department has drawn on available statistical data to identify areas of high relative need and to target specific populations within communities in line with government priorities. The expansion of the program from 2011 was supported by the development of an appropriate implementation approach which included strategies for stakeholder communication and consultation along with details of site priorities, development of new service delivery models and funding levels for each service site. Timetables setting out the sequenced implementation of the expansion were developed and revised to reflect actual implementation experience, program resources and changing program priorities.
15. The Commonwealth Grant Guidelines (CGGs) provide the Australian Government’s overarching framework for the management of grant programs by agencies, and agencies are required to advise Ministers of the requirements of the CGGs when Ministers are making decisions in relation to the awarding of grants. The TCC Program predates the introduction of the CGGs, which were first issued in 2009 and revised in 2013. However, FaHCSIA has in most key respects aligned its management of the program to the requirements of the CGGs.
16. The CGGs emphasise the benefit of undertaking competitive merit‑based selection processes as a better practice approach to consistently and transparently selecting grant recipients. The CGGs also recognise that there are circumstances when other selection processes may be appropriate, although agencies are expected to provide clear justification for not using competitive merit-based selection processes. Since the introduction of the program in 2006, FaHCSIA has made use of a combination of competitive grant selection processes as well as restricted and direct selection processes to select new providers and extend the funding agreements of existing providers.
17. While the CGGs emphasise the use of competitive merit-based selection processes, this same emphasis is not reflected in FaHCSIA’s TCC Program guidelines. Further, in advising the Minister, FaHCSIA provided justification for the use of restricted and direct selection processes but did not include explicit advice on the preference in the CGGs for competitive merit-based selection processes or the impact that alternative approaches may have on the opportunities for other organisations to access grant funding opportunities.
18. Assessing the overall impact of the program is a challenging process given the individual nature of mental illness, and that the program is providing localised and specialised services in a range of different locations. Currently FaHCSIA assesses program performance in terms of the overall numbers of people accessing the funded services. This is supported by performance information relating to client satisfaction and client progress against personal goals, where this is relevant. Information on the use of services by Indigenous clients and those from culturally and linguistically diverse (CALD) backgrounds is also collected by FaHCSIA. To assist in further understanding the effectiveness of the program FaHCSIA has undertaken a comprehensive evaluation, the results of which were released in May 2011. However, there is currently limited regular information available on the specific contributions made by the three service streams to improvements in community level mental health. FaHCSIA has reviewed its performance framework for the TCC Program and is making changes which will take effect from July 2014. Integral to the proposed revised performance framework is the continuation of periodic program evaluations.
19. The majority of funding agreements with providers under the TCC Program expire in June 2014. In planning for any subsequent grant rounds, it will be important for the department to give appropriate consideration to the preference of the CGGs for competitive processes and the opportunities these afford to improve accessibility to grant funding. FaHCSIA is also currently implementing reforms to its departmental-wide approach to the administration of grant programs. There are opportunities to support a greater focus on competitive processes at appropriate intervals and the ANAO has made one recommendation in this respect.
Key findings by chapter
Program planning and management (Chapter 2)
20. Over the period 2006–11 FaHCSIA made a number of adjustments to the TCC Program to reflect implementation experience and increased understanding of different needs for mental health services. The expansion of the program announced in 2011 is aiming to build on this base by expanding sites and the capacity of services. It further sought to refine the service delivery models and introduce program enhancements. In developing these enhancements, FaHCSIA has actively drawn on its own experience and that of service providers in the sector.
21. To support the expansion of the TCC Program, FaHCSIA has given appropriate consideration to key aspects of planning and administration. A detailed implementation plan was developed and covered essential elements such as: stakeholder consultation and communication; the development and refocusing of services models; the identification of risks; staged provider selection processes and the identification of high priority areas in which the expansion should be focused.
22. FaHCSIA has given appropriate attention to identifying areas with the greatest need for community-based mental health services such as areas with poorer socioeconomic conditions as these areas tend to have a greater incidence of mental illness than other areas.13 Accordingly, to support the program’s initial implementation and subsequent expansion, FaHCSIA has used data from the Australian Bureau of Statistics to identify areas of relative disadvantage14 and to target groups such as Indigenous Australians, CALD groups and homeless people.
23. In June 2012 FaHCSIA was funding 201 service providers in 424 locations across Australia. The program’s widely dispersed and community‑based service delivery model requires clarity in the respective roles and responsibilities of FaHCSIA’s national, state and territory offices and of the service providers. FaHCSIA’s Common Business Model for Grants Management allocates the day to day management of service providers to FaHCSIA’s state and territory offices while the overall administration and development of the program is the responsibility of FaHCSIA’s national office. Funding agreements are in place with service providers which clearly set out their roles and accountabilities. Overall, the department’s management arrangements provide a sound framework to support the ongoing administration of the program. The service providers interviewed as part of the audit considered the program was generally well managed from their perspective.
Grant Assessment and selection (Chapter 3)
24. The CGGs, while noting that several selection methods are open to Australian Government agencies, indicate the Australian Government’s preference for using open competitive merit-based selection processes when selecting grant recipients. Where an alternative method is chosen as the most appropriate to the circumstances, the CGGs emphasise that the selection methods need to promote transparent and equitable access to grants and that agreement on the process needs to be given by the Minister, chief executive or appropriate delegate. FaHCSIA informed the ANAO that a competitive merit-based grant process was the department’s starting position for TCC Program grant rounds.
25. FaHCSIA has primarily undertaken open competitive merit-based selection processes to initially select service providers but has also made use of direct and restricted competitive processes in situations where the objective of the selection process was to support an expansion of existing services. Direct selection processes have also been used to extend a large number of existing funding agreements to align their expiry dates, with the result that most current providers have had their funding agreements renewed without a competitive process. The use of various selection processes is provided for in the FaHCSIA TCC program guidelines and Ministerial approval has been obtained in all cases in relation to the proposed selection methods.
26. Under the CGGs, agencies are required to advise Ministers of the requirements of the guidelines. This will necessarily involve advising on the policy aspects and obligations set out in the Financial Management and Accountability Regulations 1997.15 Briefs provided by FaHCSIA to the Minister seeking approval did not routinely include reference to the CGGs, and in this context the preference for competitive merit-based selection processes. FaHCSIA’s TCC Program guidelines also do not reflect the emphasis given in the CGGs to competitive merit-based selection processes. The TCC Program guidelines16 list three possible selection methods but indicate that the choice of method is at the discretion of the department.
27. Under broader reforms, the Australian Government has committed to strengthening the contribution of the not-for-profit sector to the government’s social inclusion agenda.17 Streamlining contracting and funding arrangements are part of the overall reform approach but the government is also seeking to improve the sector’s accessibility to grant funding opportunities. Open competitive selection processes would be expected to help in this regard, and it is important that agencies give appropriate consideration to ways of increasing access to grant opportunities, and that decision makers are advised accordingly.
Reporting and monitoring (Chapter 4)
28. There is limited information available on the specific contributions made by PHaMs, FMHSS and MHR: CS to improvements in community level mental health. Assessing the overall impact of the TCC Program is challenging and FaHCSIA recognises the limitations of its current performance management framework. As part of ongoing program management and continuous improvement, in September 2010, the department reviewed the program’s existing performance management information collections and its needs for future planning and monitoring. As a result of that review, the department identified the following priority activities to improve its performance framework. These are to:
- improve the capacity to report on Mental Health Reforms;
- streamline and reduce reporting demands on providers;
- prepare for the non-government-organisations’ National Minimum Data Set;
- focus on outcome reporting; and
- move to client-level data over time.
29. FaHCSIA is taking important steps in the review of its current performance management framework. A draft framework was completed in 2011 and FaHCSIA undertook a pilot of its use with service providers. The department needs to maintain momentum to ensure its implementation by mid 2014. Once it is in place the new framework will assist FaHCSIA to better monitor the ongoing service performance of providers and to access higher level information required to report against outcomes and program objectives.
Summary of agency response
30. FaHCSIA provided a formal response to the audit which is contained in full in Appendix 1. A summary of FaHCSIA’s response was also provided:
It was beneficial for the Department to be involved in the audit during its peak phase of implementing new community mental health services nationally.
The Department provides comprehensive advice to the Minister in relation to grants selections and approvals. The Department’s current Delivery Reform Agenda will provide opportunities to further strengthen advice to systematically provide explicit reference to the Commonwealth Grant Guidelines.
The Department’s approach to continuous improvement through implementing a strengthened performance framework will assist in ensuring greater information is available on the impacts of the Targeted Community Care (Mental Health) Program.
Recommendations
|
Recommendation No. 1 Paragraph 3.14 |
In order to better support the Minister in relation to grant funding decisions, the ANAO recommends that FaHCSIA provides more explicit advice to the Minister on key aspects of the Commonwealth Grants Guidelines and that agency staff are better supported in providing this advice. |
|
|
FaHCSIA’s response: Agreed. |
Footnotes
[1] Australian Institute of Health and Welfare, 2007. The burden of disease and injury in Australia, AIHW, Canberra. Levels of death and disability from a comprehensive set of diseases, injuries and risks to health are combined to measure the total health ‘burden’. Following cancers and cardiovascular diseases mental disorders are the third leading cause of overall disease burden in Australia, accounting for 13.1 per cent of Australia’s total burden of disease and injury.
[2] COAG National Action Plan for Mental Health 2006–2011, Fourth Progress Report covering implementation to 2009–10, May 2012, p. 16.
[3] Department of Families, Housing, Community Services and Indigenous Affairs, Targeted Community Care (Mental Health) Program Guidelines, Part A –June 2011, p. 6.
[4] Australian Bureau of Statistics, National Survey of Mental Health and Wellbeing: Summary of Results, 2007, cat. no.4326.0, Canberra.
[5]The Mental Health of Young People in Australia, Sawyer et al, Mental Health and Special Programs Branch, Commonwealth Department of Health and Aged Care, 2000.
[6] Mental Health Council of Australia, Not For Service: Experiences of Injustice and Despair in Mental Health Care in Australia, Canberra, 2005. The Senate, Select Committee on Mental Health, A National Approach to Mental Health – From Crisis to Community, Final Report, April 2006.
[7] COAG National Action Plan for Mental Health 2006–2011, 14 July 2006. http://archive.coag.gov.au/coag_meeting _outcomes/2006-07-14/docs/nap_mental_health.pdf [accessed 15 January 2013].
[8] ibid.
[9] Families, Housing, Community Services and Indigenous Affairs, Portfolio Budget Statement 2012–2013, p. 94. http://resources.fahcsia.gov.au/budget/2012-13/FaHCSIA_PBS_2012-13.pdf [accessed 5 February 2013].
[10] Department of Families, Housing, Community Services and Indigenous Affairs, Targeted Community Care (Mental Health) Program, Part A: Program Guidelines, November 2012.
[11] Originally known as Mental Health Community Based.
[12] Originally known as Mental Health Respite.
[13] Australian Bureau of Statistics, Measures of Australia’s Progress, 2010, cat no. 1370.0, Canberra.
[14] Socio-Economic Indexes for Areas (SEIFA) Index of Disadvantage. The SEIFA is based on National Population Census data. Australian Bureau of Statistics, 2039.0 – Information Paper: An introduction to Socio-Economic Indexes for areas (SEIFA) [Internet], ABS, Australia, 2006, http://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/2039.02006? OpenDocument [accessed 25 February]. SEIFAs based on 2011 Census data had not been released at the time of the audit.
[15] ANAO, Audit Report No. 21 2011–2012, Administration of Grant Reporting Obligations, p. 47.
[16] Department of Families, Housing, Community Services and Indigenous Affairs, Targeted Community Care (Mental Health) Program, Part B:Information for Applicants, November 2012.
[17] Australian Government Initiative, National Compact, working together, part of the social inclusion agenda. http://www.nationalcompact.gov.au/ [accessed 10 January 2013].