Browse our range of reports and publications including performance and financial statement audit reports, assurance review reports, information reports and annual reports.
Auditor-General Report No. 41 of 2005–06
Administration of Primary Care Funding Agreements
Published
Wednesday 24 May 2006
Portfolio
Health and Ageing
Entity
Department of Health and Ageing
Sector
Ageing
Health
The audit objective was to assess Health's administration of primary care funding, with a focus on the administrative practices of the Primary Care Division and Health's State and Territory Offices. In forming an opinion on the audit objective, the ANAO reviewed 41 agreements, with a combined value of $252 million. The ANAO also reviewed relevant documentation and files, interviewed programme officers and met with a number of stakeholders. The audit comments on a range of issues, including the utility of funding agreements, monitoring, payments, and support for administrators.
Summary
Background
The primary care sector, comprising general practice, nursing, allied health, community health and community pharmacy, is the most commonly accessed part of the health system.
Accessing primary care typically encompasses a visit by a person to their general practitioner to seek treatment for illness. However, primary care services are also provided by other medical professionals working outside of general practice, such as immunisations provided within a community health setting.
It is through the primary care sector, predominantly general practice, that Australians access a range of diagnostic, pharmaceutical and acute care services. Acute care involves the provision of medical and other services in hospitals as well as specialist services in the community.
A strong primary care system is a key to providing quality care in the treatment of illness and in the prevention of health problems through early intervention. Research has shown that:
…countries with well-developed systems of primary care, such as Australia, achieve better health outcomes at less cost. Conversely, countries with very weak primary care infrastructures have poorer performance in major aspects of health. 1
The nature of primary care has been changing as governments and providers in developed countries respond to demographic and morbidity changes, particularly due to the impact of ageing populations. There has also been a major focus on controlling costs while continuing to meet increasing societal needs and expectations.
In February 2006, the Council of Australian Governments announced a $1.1 billion funding package aimed at achieving better health for all Australians, through better health promotion, prevention and early intervention strategies.
The Department of Health and Ageing (Health) has a central role in supporting changes in primary care in Australia. Health's Portfolio Outcome 4: Primary Care works towards strengthening the primary care sector to ensure all Australians have access to high quality, well-integrated and cost-effective primary care. Outcome 4 is managed within the Department by the Primary Care Division (PCD or the Division). In 2005–06, the Australian Government's total administered items2 appropriation for the primary care outcome is $816.9 million, with $30.4 million appropriated for departmental items.3
Health does not provide primary care services directly to health consumers, instead it contributes to strengthening of the sector through funding4 primary care programmes. Health distributes funding via agreements with a range of organisations, such as universities, other education providers, private sector organisations and representative bodies. On 30 June 2005, PCD and Health's State and Territory Offices (STOs) were administering approximately $895 million5 in primary care funding via 389 funding agreements. These agreements range in size from $1800 to $150 million and in duration from five weeks to around six years.
This financing supplements other primary care moneys, such as the $10.6 billion in funding for Medicare services and $6.3 billion in funding for the Pharmaceutical Benefits Scheme.
PCD funds a variety of primary care activities under 26 programmes and initiatives (see Figure 1 for a snapshot of two programmes). A large number of these programmes involve developmental work, such as establishing after hours medical services, trialling of new approaches to treat chronic disease through general practice, and building primary care research capacity. These types of activities require agreements with sufficient flexibility while providing adequate levels of control to ensure that the Department ‘gets what it pays for'.
Figure 1 Snapshot of primary care programmes
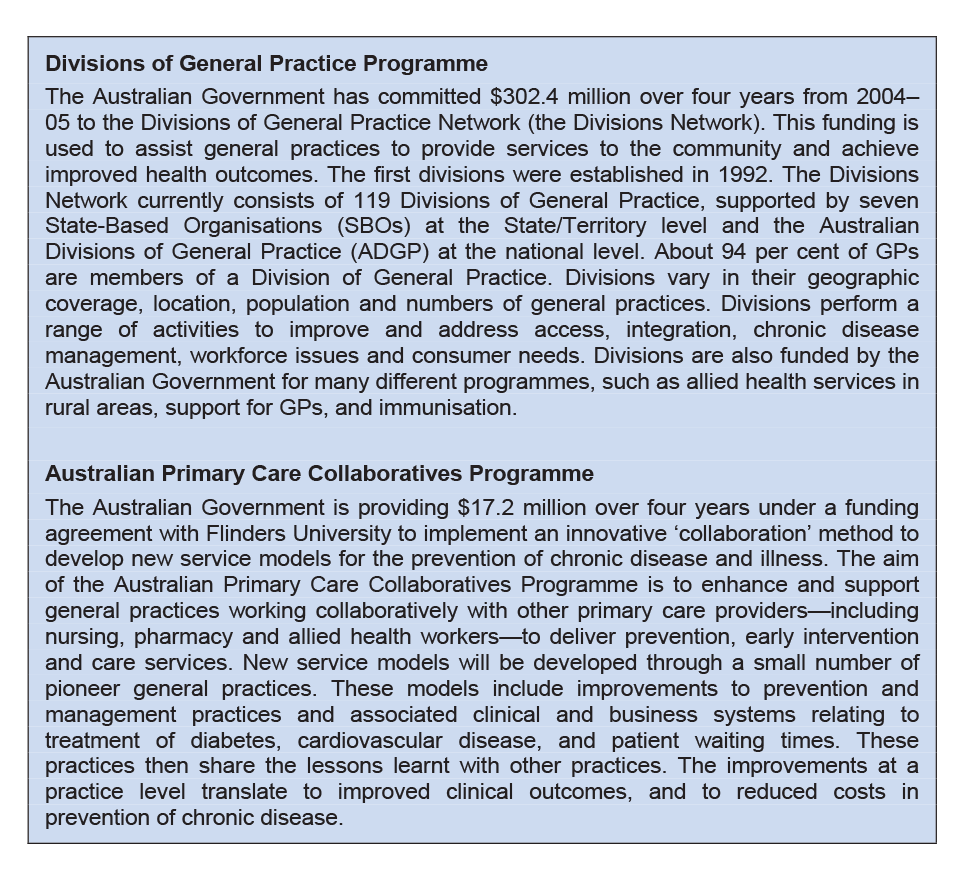
Source: Health and the Australian Divisions of General Practice
Audit overview
The audit objective was to assess Health's administration of primary care funding, with a focus on the administrative practices of the Primary Care Division and Health's State and Territory Offices. In forming an opinion on the audit objective, the ANAO reviewed 41 agreements, with a combined value of $252 million. The ANAO also reviewed relevant documentation and files, interviewed programme officers and met with a number of stakeholders.
The audit comments on a range of issues, including the utility of funding agreements, monitoring, payments, and support for administrators.
Key findings
Funding agreements (Chapter 2)
Programme officers use standard funding agreements developed by Health's Legal Services Branch. The standard agreements include appropriate general terms and conditions, such as clauses linking payments to performance. Where programme officers make changes to the general terms and conditions, these are based on legal advice.
While the general terms and conditions in standard funding agreements are appropriate, the performance specifications in schedules developed by programme areas are not always clear. This is partly explained by the difficulty in establishing specifications for developmental work and the need for agreements with sufficient flexibility. Notwithstanding, clear standards/targets provide guidance to programme officers and funded organisations and reduce the risk of disputes.
Agreements commonly contain ambiguous activity descriptions, insufficient budget detail, and unclear reporting obligations. Furthermore, timelines for funded primary care activities are not aligned to reporting periods and the use of targets to define performance expectations is limited. These issues lessen the usefulness of funding agreements to programme officers and funded organisations when determining satisfactory performance.
Health does not ensure that all primary care funding agreements are signed before the project period and/or the activity has begun. Delays in the signing of agreements increase the risk of disputes as the terms, conditions and performance expectations may not be agreed before work begins.
Monitoring (Chapter 3)
The limited use of activity plans and/or standards/targets in funding agreements means that programme officers do not have a ‘yardstick' against which an objective assessment of performance can be made. Consequently, programme officers primarily rely on their experience and judgement to determine whether reported performance is satisfactory. This approach poses problems for the consistent implementation of programmes, particularly where there are changes in administrative staff, or where there is variability in the skills and knowledge of programme officers administering national programmes.
Health does not, in general, document the assessment of progress reports from organisations funded under primary care agreements, including the analysis of progress and financial data, to record the basis on which it has determined the performance of funded organisations. Limited documentation of decisions affects Health's ability to justify its funding actions and to ensure that it has met agreement obligations. It also makes management more difficult as there is no history of events and key decisions.
The system used by Health to monitor primary care funding agreements relies primarily on self-reporting, with limited activity to verify the accuracy or quality of information within reports submitted by funded organisations. Some level of review encourages accuracy in reporting and increases the confidence in the quality of information reported by funded organisations.
In general, Health incorporates changes into primary care funding agreements through written variations. However, the timing of variations to extend agreements is problematic, with the parties commonly executing variations after the original agreement has ended. Where work continues ‘between' the end of the project period in the original agreement and the commencement of the project period under the variation, there is an increased risk of disputes. That is because of the lack of clear authority to continue work, and increased uncertainty surrounding the terms and conditions that apply to this work.
The general terms and conditions in the standard funding agreement, prepared by Health's Legal Services Branch, establish obligations on agreement parties that need to be regularly monitored, for example, maintenance of sufficient insurance coverage. Programme officers are not, however, reviewing these terms and conditions to inform their monitoring practices. As a consequence, programme officers have overlooked some obligations.
Health is working to address problems with the sharing of administrative responsibility for funding agreements between its Central Office and STOs. Initiatives stemming from a recent review are aimed at improving the way in which programmes are coordinated and delivered. Notwithstanding, there is currently a lack of clarity surrounding the role of PCD and STOs in the day-to-day administration of agreements. The way in which PCD has allocated administrative responsibility to STOs has resulted in inadequate sharing of information on jointly administered agreements and, in at least one instance, unclear responsibilities for agreement administration.
Payments (Chapter 4)
Health has procedures that cover payments under funding agreements. There is, however, a limited awareness of the procedures among programme officers, with work areas developing their own payment documentation and complementary processes. The development of documentation for standard administrative practices by work areas, such as payment request forms, increases costs and has led to issues of non-compliance with the Chief Executive's Instructions.
In spite of weaknesses in assessment practices, programme officers authorised payments that were in accordance with the amounts in funding agreements and, in the majority of cases, within the time allowed.
Support for administrators (Chapter 5)
Health has established a set of policies and procedures, both at the departmental and divisional level, to guide funding activities. While this guidance covers all stages of the funding process, there is scope to increase guidance for programme officers in order to address current issues relating to the lack of clarity and comprehensiveness of performance specifications in agreements. Further, the lack of programme-specific guidance for some programmes, to supplement departmental and divisional guidance, has led to inconsistencies in the delivery of national programmes, such as different criteria/methods used to assess reports.
Programme officers have ready access to legal and technical specialists, both at the departmental and divisional levels. These specialists provide advice and assistance on matters such as the type of agreement to select, amendments to the standard funding agreement and risk management approaches. Health has also reviewed its approach to the provision of technical advice, and is currently establishing a new model to deliver local level advice to staff across the Department.
Health has established a process to identify the development needs of staff. In response to needs identified through this process, the Department has established a standard suite of training courses designed to equip staff with an understanding of their rights and obligations when dealing with parties to funding agreements. Health also provides tailored training to officers administering funding agreements. Participation in courses by programme officers with responsibility for managing primary care agreements is, however, patchy with a number of officers not having attended training for many years.
There are two registers used within the Department to manage primary care agreements. The limited utility of the central contracts register means that a supplementary PCD Register is used to support monitoring and reporting requirements. The use of multiple registers to record PCD agreements is problematic as different areas of the Department use different data to inform agreement monitoring and reporting. This has contributed to the reporting—both internally and externally—of incorrect agreement information. The use of supplementary systems is less efficient, more costly and increases the risk of data integrity issues. Health has advised that it is aware of the issues associated with the reporting of contract information, and is actively addressing these issues through the ongoing improvements to the guidance frameworks and systems.
Health is implementing a programme management information system to provide greater assistance to programme officers in the day-to-day administration of funding agreements. Health plans to implement the proposed system by July 2009. In the interim, programme officers continue to use ad hoc, stand-alone approaches, such as spreadsheets and to-do lists. The use of these systems is less efficient and costs more. The risk that a contractual obligation is overlooked, particularly where a programme officer is absent or where there is a new programme officer, is also increased. Health envisages that the proposed system will reduce these risks.
Overall audit opinion
The aim of the Government's primary care funding is to ensure all Australians have access to high quality, well-integrated and cost-effective primary care. The manner in which Health administers primary care funding is an important factor in realising this aim.
Health is well advanced in establishing guidance and training to equip its officers with the skills and knowledge needed to effectively administer funding agreements. Health is working to strengthen its approaches, with the development of an information system to support day-to-day agreement administration. This system will complement existing contract registers that Health uses to monitor agreement activity and to inform internal/external reporting. Aspects of Health's day-to-day administration of primary care agreements, such as payments, are also generally consistent with agreement requirements.
Notwithstanding, there are aspects of primary care agreement administration that require strengthening in order for Health to demonstrate that it ‘gets what it pays for' and to improve the efficiency of administration.
At present, the specification of performance expectations in primary care funding agreements is insufficient, with limited use of clearly expressed and appropriate activity plans and/or standards/targets against which performance can be objectively assessed. There are also weaknesses in the documentation of decisions, particularly relating to the assessment of reports, which affect Health's capacity to demonstrate effective performance management.
The absence of a programme management information system, problems surrounding the management and use of contract registers, and unclear arrangements for the sharing of agreement administration between PCD and State and Territory Offices (STOs) have also led to less efficient administration.
The ANAO made three recommendations to improve Health's administration of primary care funding.
Health's response
The Department is supportive of the audit and its findings, and agrees with the recommendations, noting that they apply specifically to aspects of the administration of primary care funding, and not to the operations of the Department as a whole. The Department has a number of initiatives in hand to improve the administration of primary care funding agreements in response to the ANAO recommendations.
Health also provided a response to each of the recommendations. These appear immediately following each recommendation in the body of the report.
Footnotes
1 Department of Health and Ageing, 2005, General Practice in Australia: 2004, Canberra, p.4, viewed 1 March 2006, http://www.health.gov.au/internet/wcms/publishing.nsf/Content/pcd-publications-gpinoz2004>.
2 Administered items are those assets, liabilities, revenues and expenses controlled by the Government and managed or overseen by agencies or authorities on behalf of government.
3 Departmental items are those assets, liabilities, revenues and expenses controlled by agencies or authorities and used in producing their outputs.
4 Health has defined funding as ‘…the process whereby the Department allocates money to support the achievement of health and ageing objectives within the community (i.e. the Department is not the primary beneficiary).' According to the Department, a funding agreement differs from a contract for a service/consultancy as funding encompasses the performance of ‘specified activities for a set price', whereas a contract for a service/consultancy is defined as ‘getting the best price for an activity.'
5 The total value of administered agreements ($895 million) is greater than the annual Outcome 4 appropriation ($816.9 million) as many agreements span several years. It should also be noted that the annual appropriation is not used exclusively for funding programmes. A proportion of the appropriation is used for the contracting of goods/services/advice, as well as alternative financing of primary care, such as incentive payments to GPs through Medicare.