This chapter examines the development of the 5CPA, including the planning, costing and negotiation of the agreement.
Introduction
2.1 The Department of Health (Health) has developed and negotiated successive community pharmacy agreements on behalf of the Australian Government. This chapter examines Health’s processes for planning, costing and negotiating the Fifth Community Pharmacy Agreement (5CPA) with the Pharmacy Guild of Australia (Pharmacy Guild), including:
- planning, with particular reference to the development of a 5CPA costing model by Health;
- the forecasting and reporting of expected 5CPA costs and savings; and
- the negotiation of the 5CPA and outcomes of negotiations.
Planning for the 5CPA
2.2 Health advised the ANAO that there was no clear start date for its planning of the 5CPA, as there was a gradual ‘ramping up’ of activity that started at least 12 months before negotiations with the Pharmacy Guild commenced in July 2009. Although there was no documented plan for Health’s development of the 5CPA, Health advised the ANAO that the key steps in the process were:
- background research;
- the development of a forecasting model to estimate the costs of pharmacy remuneration under different scenarios;
- engagement with the department’s senior executive;
- seeking government approval; and
- negotiations with the Pharmacy Guild.
2.3 Health further advised the ANAO that the department engaged more widely beyond the department’s senior executive, including across the department, through an inter-departmental committee, and other stakeholder groups beyond the Pharmacy Guild.
Background research and analysis
2.4 Health indicated that the 5CPA planning process involved consideration of evaluations of the components of the 4CPA. One evaluation was completed before the 5CPA was signed, and eleven were completed afterwards. To fully inform the development of the agreement, the evaluations should desirably have been completed before the agreement was finalised. In this respect, Health advised the ANAO that:
Evaluations and/or reviews undertaken during 4CPA, including those that did not commence until 2010, were still used to inform the construct of 5CPA programs (i.e., how continuing programs may have been implemented). In several instances, the Department used draft reports (if they existed) as a part of the negotiations.
2.5 In October 2008, Health convened a Departmental Workshop Group that canvassed a range of strategic and policy issues related to the development of the 5CPA. In November 2008, Health also convened a Remuneration Working Group to conduct background research for the development of the 5CPA. Following research and analysis of pharmacy’s role in the health care system, Health concluded that the current system of remunerating pharmacies based on the price and volume of medicines that they dispense had significant drawbacks. Health advised the ANAO that:
The results of the Department’s research and analysis were presented and discussed at an Inter-Departmental Committee (IDC) consisting of officers from the Departments of Finance and Deregulation, the Treasury, the Prime Minister and Cabinet and Industry, Tourism and Resources. Following the Department’s research and analysis and the consideration of the IDC, it was concluded that the current system of remunerating pharmacies based on the price and volume of medicines that they dispensed had drawbacks consistent with any fee-for-service or retail model, namely:
- the cost of pharmacy remuneration was driven by factors unrelated to health outcomes for patients, or services provided to patients; and
- retail pharmacies had limited incentive to improve the quality use of medicines, or other professional services to consumers.
2.6 Health did not keep a record of the meetings of the inter-departmental committee that considered these issues in the lead up to the negotiation of the 5CPA.
2.7 Pharmacy remuneration is structured around the price of individual medicines through a complex system of mark-ups and fees, which do not necessarily relate to the level of professional service required by different patients with different medication regimens. Health’s records indicate that, at the time, the department considered the negotiation of the 5CPA to be an opportunity to improve health outcomes through better utilisation of the professional skills of pharmacists. Health considered that these outcomes could be achieved by restructuring pharmacy remuneration to shift the financial incentives from the volume driven sale of medicines, to the delivery of professional services.
Development of the 5CPA costing model
Limitations of previous costing model
2.8 A key departmental objective in the lead up to the negotiation of the 5CPA was the development of a pharmacy remuneration costing model. Health had experienced difficulties in negotiating the 4CPA partly due to a lack of technical capability. According to a departmental report:
Unfortunately, the Department had to rely on an Excel spreadsheet to forecast the costs to government of the various remuneration scenarios put forward during the negotiations of the Fourth Agreement. The Excel spreadsheet could only provide linear forecasting, relied on manual manipulation of data (therefore subject to human error), was dependent on availability of Departmental staff with advanced Excel skills and struggled to manage the large amount of Medicare PBS dispensing data. The Excel spreadsheet was slow and cumbersome. The deficiencies of the Excel spreadsheet were again highlighted in the 2006–07 negotiations of the compensation package to pharmacists under the PBS reforms…
2.9 The shortcomings of Health’s Excel spreadsheet re-emerged in 2006–07 when the Government introduced Price Disclosure for certain PBS items, in order to align their prices with actual market prices, as outlined in Figure 2.1.
Figure 2.1: Price Disclosure
|
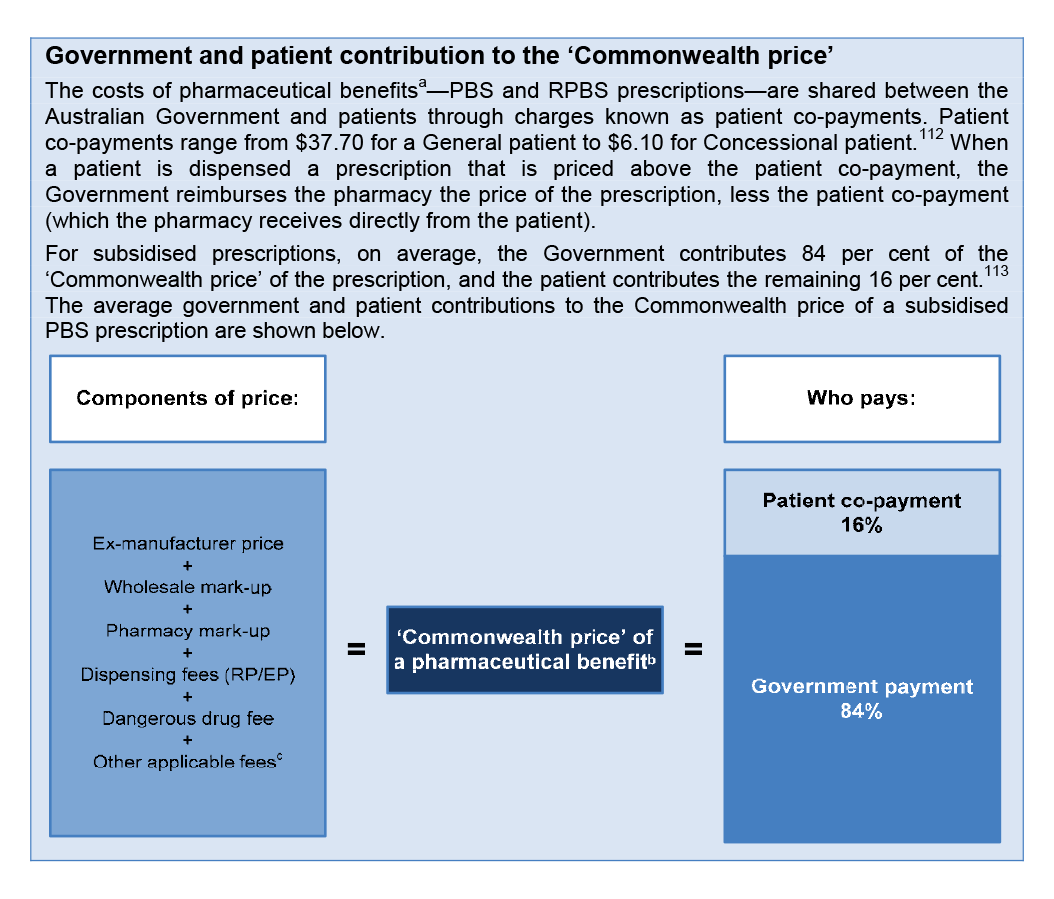
Manufacturers may sell PBS medicines to wholesalers and pharmacies at less than the ex-manufacturer price agreed with the Australian Government. In 2007, the growing disparity between the government price and the market price of PBS drugs led to the introduction of mandatory Price Disclosure for some drugs. Under Price Disclosure arrangements, manufacturers are required to report the actual price and sales volumes for certain PBS drugs (generally those off-patent). Under the 2007 Price Disclosure rules, if the weighted average manufacturer discount was 10 per cent or more over a 12 month period, the government price was reduced to the average market price. However, at that time, the reduction in government price did not take effect until 24 to 28 months from the start of data collection.a
Price Disclosure produces savings in two ways:
- by reducing the ex-manufacturer price (the price of the medicine); and
- by reducing the wholesaler mark-up and pharmacy mark-up (which are either a percentage or flat fee, depending on the price of the medicine).
Price disclosure directly affects pharmacy remuneration as pharmacies receive higher remuneration for more expensive medicines because the wholesale mark-up and pharmacy mark-up are generally based on a stepped percentage mark-up of the relevant base price, and are only capped at a flat fee for the highest price bracket.
|
Source: ANAO analysis of Department of Health information.
Note:
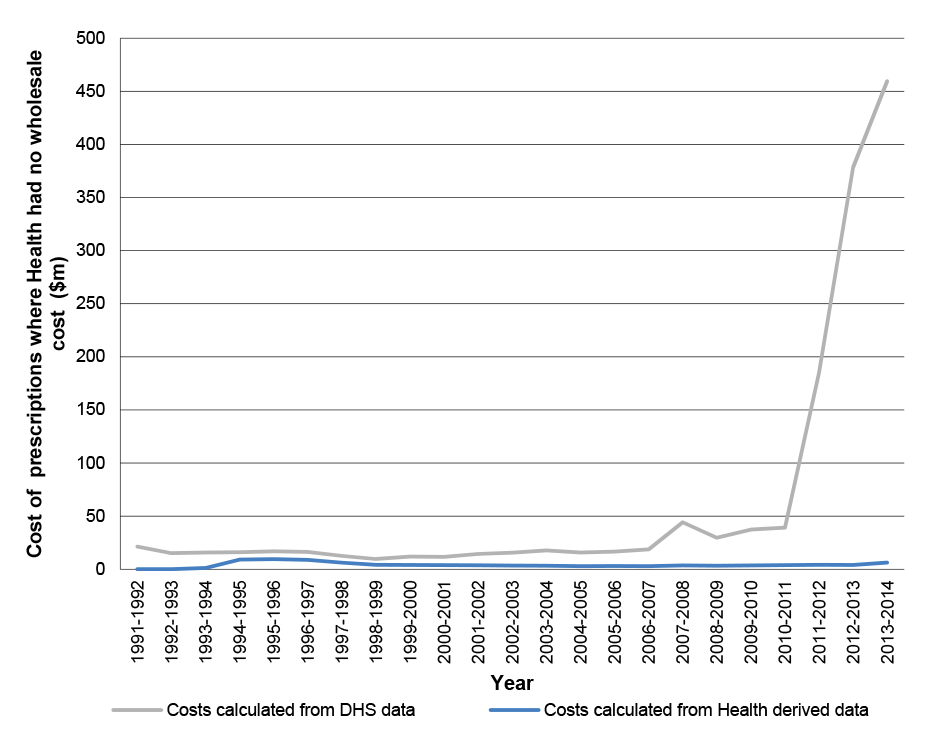
2.10 Health had relied on the Excel spreadsheet when negotiating a structural adjustment package (financial assistance) to assist pharmacies transition to the new Price Disclosure arrangements. Health reported the following outcome of negotiating the structural adjustment package with the Pharmacy Guild:
… The Commonwealth and the Guild arrived at a significantly different figure for the dispensing fee adjustment required to achieve the agreed compensation package. A review of the Excel spreadsheet highlighted significant errors in the manual manipulation of PBS dispensing data. The Department therefore agreed with the Guild to rebuild its remuneration model, and recalculate the dispensing fee amount within a six month timeframe.
2.11 By 2009, Health was also considering options for expanding Price Disclosure to bring the government price for medicines closer to the actual market price. In addition, the 5CPA negotiations were expected to canvass changes to the components of pharmacy remuneration. Consequently, Health needed to develop a costing model in order to accurately forecast:
- the cost of pharmacy remuneration under different scenarios (such as a different professional fee structure); and
- savings from expanded Price Disclosure.
2.12 Health advised the ANAO that its new costing model, called the Pharmacy Remuneration and Negotiation Cost Information System (PhRANCIS), was developed for 5CPA costings and due to its capabilities it could also be used to forecast savings for different Price Disclosure scenarios.
Forecasting pharmacy remuneration
2.13 In planning for the 5CPA, Health advised that it employed its new costing model as follows:
PhRANCIS forecast prescription volumes using historical data and derived a base average ex-manufacturer price using the known wholesale mark-up, pharmacy mark-up, dispensing fee and dangerous drug fee applicable at a point in time before the negotiations started. It [PhRANCIS] then used the script forecasts and base ex-manufacturer prices for medicines to apply expected price changes and other remuneration components under various costing scenarios, including Further PBS Reforms [revised Price Disclosure arrangements].
2.14 Under PBS arrangements, public and private hospitals approved under Section 94 of the National Health Act may claim reimbursement for dispensing pharmaceutical benefits. At the commencement of the audit the ANAO sought confirmation from Health that remuneration for hospital pharmacies was not included in 5CPA ‘community pharmacy’ remuneration. Health advised the ANAO that remuneration for s94 hospitals was not contained within the $15.4 billion funding for 5CPA.
2.15 However, the ANAO’s examination of the prescription data used to forecast 5CPA pharmacy remuneration indicated that Health:
- had used prescription data for Section 85 items from all approved suppliers (including those dispensed from public and private hospitals); and
- did not include prescription data for Section 100 items (such as Highly Specialised Drugs) dispensed from retail pharmacies.
2.16 Health’s inclusion of Section 85 items dispensed from suppliers other than retail pharmacies (including public and private hospitals) overstated forecast remuneration for retail pharmacies under the 5CPA. In contrast, Health’s exclusion of Section 100 items dispensed from retail pharmacies understated forecast remuneration for retail pharmacies from this source.
2.17 In addition, a key Australian Government objective of the 5CPA negotiations was to develop more appropriate remuneration arrangements for chemotherapy infusions. It was anticipated that chemotherapy infusions would be transferred from Section 85 to Section 100 arrangements, with higher dispensing fees. Although PhRANCIS had the capacity to model changes in remuneration for such classes of drugs—and the impact of price disclosure on those drugs—the department did not use PhRANCIS to model changes to remuneration arrangements for chemotherapy infusions.
2.18 In summary, notwithstanding the limitations of Health’s methodology, the 5CPA costing model enabled Health to forecast prescription volumes, and broadly estimate the costs of pharmacy remuneration for the 5CPA. The 5CPA baseline pharmacy remuneration was forecast by incorporating the expected price reductions that would occur under existing Price Disclosure arrangements (as established in 2007). The 5CPA model was then used to forecast pharmacy remuneration under proposed new Price Disclosure settings (proposed to be implemented in 2010).
2.19 The 5CPA costing model (PhRANCIS) forecasts the total cost of pharmaceutical benefits, including pharmacy remuneration, which is paid jointly by government and by patients. Health advised the ANAO that, in order to identify the cost to government, the total costs forecast by PhRANCIS were manually adjusted to exclude patient contributions.
5CPA costs
Treatment of patient contributions
Advice to Ministers before negotiating the 5CPA
2.20 In the lead up to the negotiation of the 5CPA, Health advised Ministers that the 4CPA was forecast to provide $11.6 billion in Australian Government funding to pharmacies and wholesalers over the five years of its operation to 30 July 2010. In October 2009, Health again advised Ministers that expenses under the 4CPA were expected to cost government $11.6 billion, and that if 4CPA arrangements continued, expenditure for the 5CPA would be just under $16.0 billion.
2.21 The ANAO analysed Health’s 2009 estimate of the cost to government of the 4CPA and the proposed 5CPA as reported to Ministers, and observed that both estimates included the value of patient co-payments, which are payments made to pharmacies by patients rather than the Australian Government. Patient co-payments are described in Figure 2.2.
Figure 2.2: Sources of funding for pharmaceutical benefits: government and patient contributions
Source: ANAO analysis.
Notes:
2.22 Including patient co-payments in cost estimates that Health provided to Ministers in August to October 2009 had the effect of significantly overstating the cost to Government of both the 4CPA and 5CPA. In the case of the 5CPA, the cost to Government was overstated by approximately $2.2 billion.
Funding obligations set out in the 5CPA
2.23 Although actual expenditure on pharmacy remuneration is demand driven—depending on the number of PBS and RPBS medicines prescribed by doctors—the 5CPA commits the Australian Government to delivering a fixed sum of money as follows:
The Commonwealth will deliver $15.4 billion under the Agreement as set out in the following table … Pharmacy remuneration: $13,771.6 million
2.24 There is no formal mechanism in place to reconcile actual expenditures on pharmacy remuneration against funding specified in the 5CPA.
2.25 The ANAO analysed Health’s final costing for pharmacy remuneration of $13 771.6 million—as incorporated in the 5CPA—and observed that it included the value of patient co-payments (approximately $2.2 billion). Health advised the ANAO that patient contributions have always been included when remuneration is reported in community pharmacy agreements, and the 5CPA included ‘the total remuneration that it delivers’. Health also acknowledged that:
This [approach] could create some confusion about the cost to Government versus the value provided from both Government and patients to pharmacy under the Agreement.
Total pharmacy remuneration delivered by the 5CPA
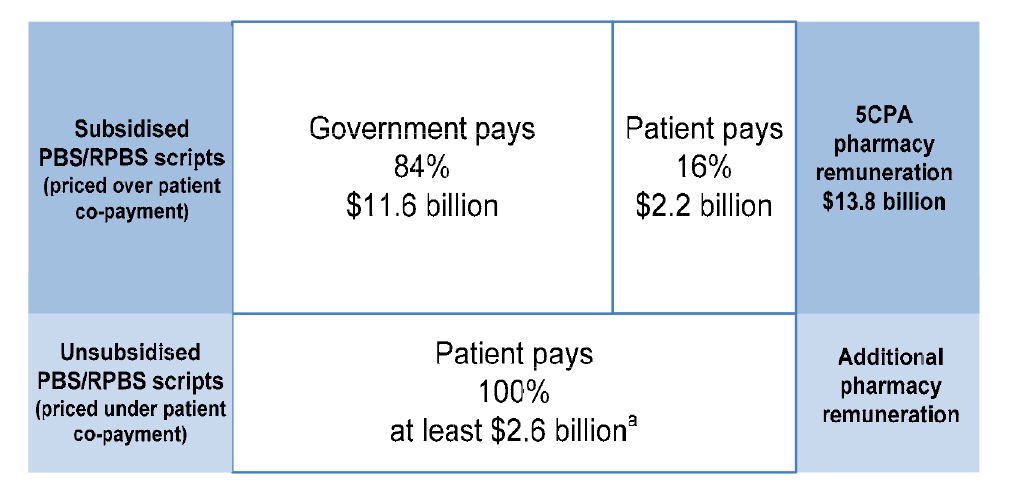
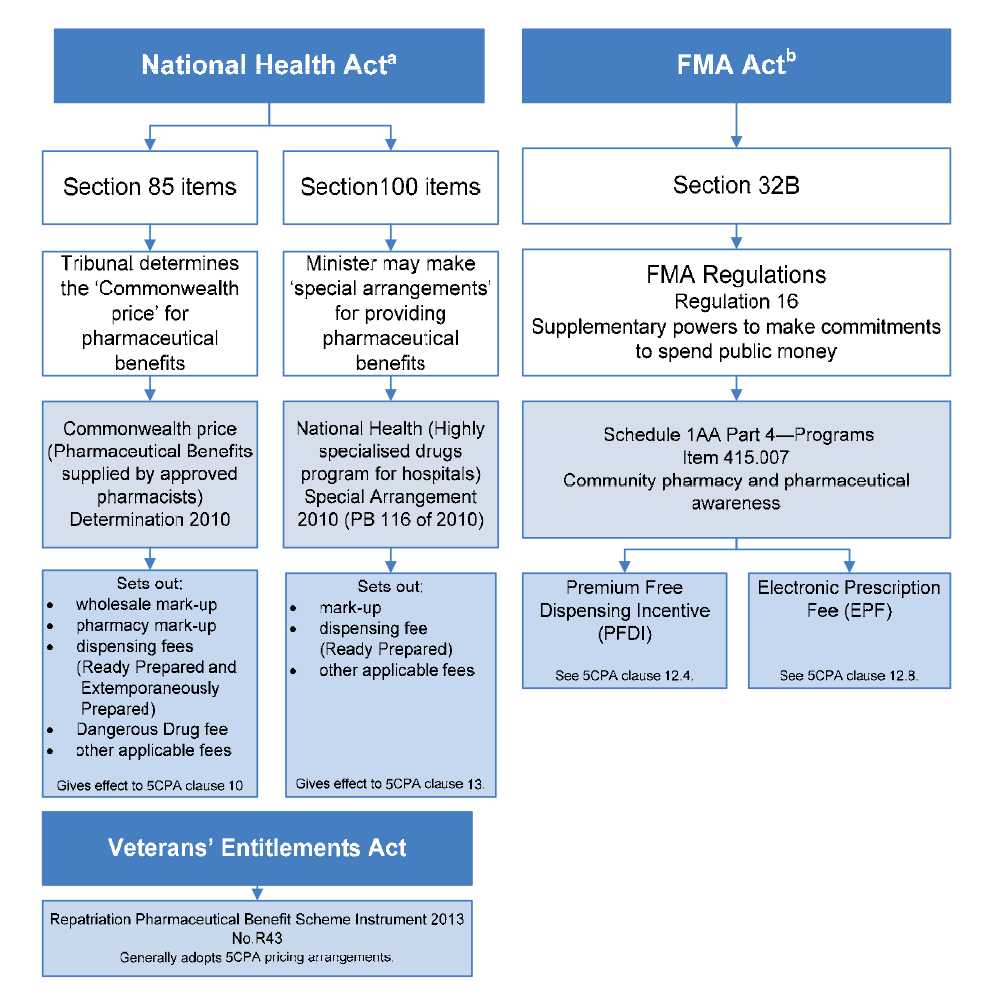
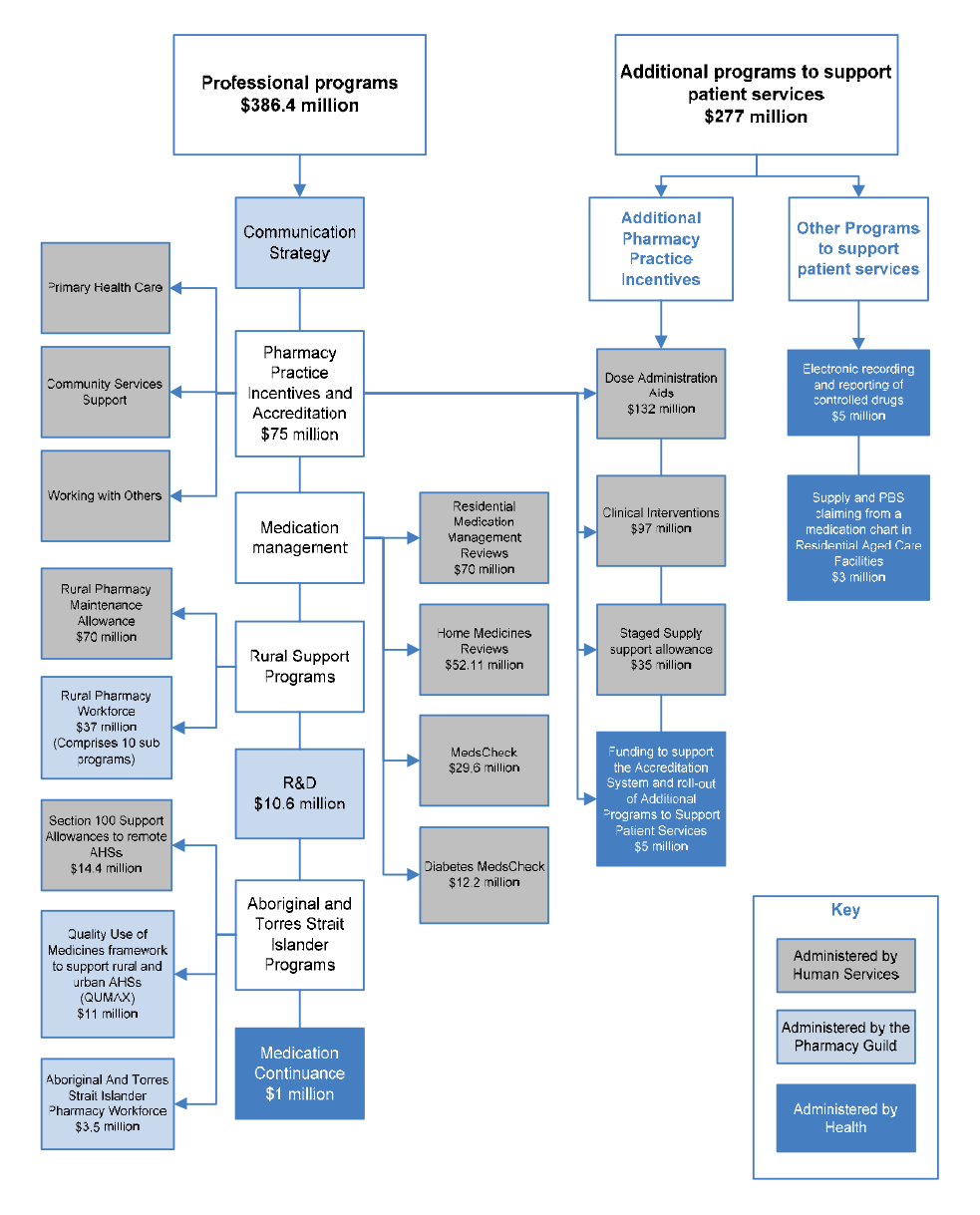
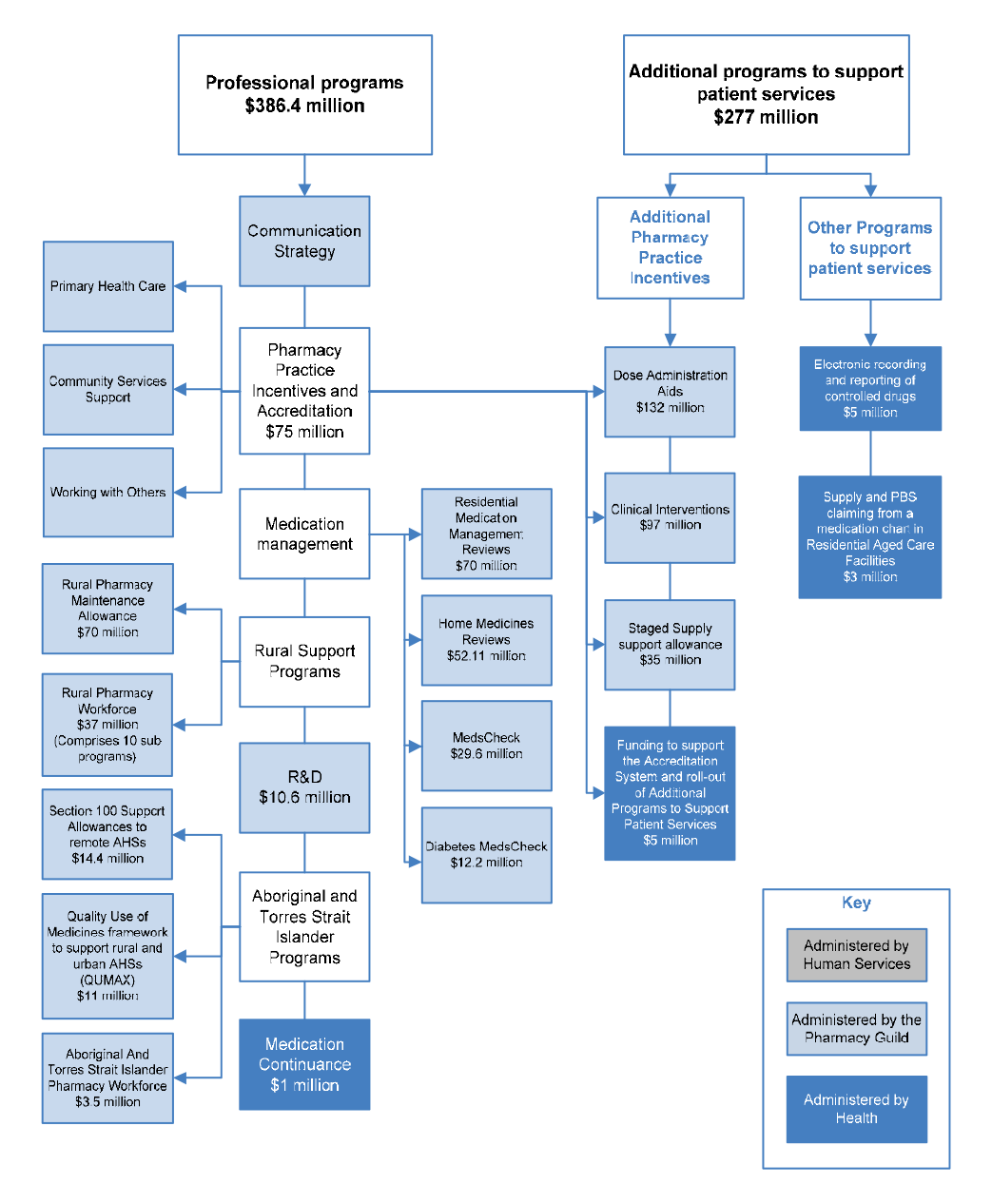
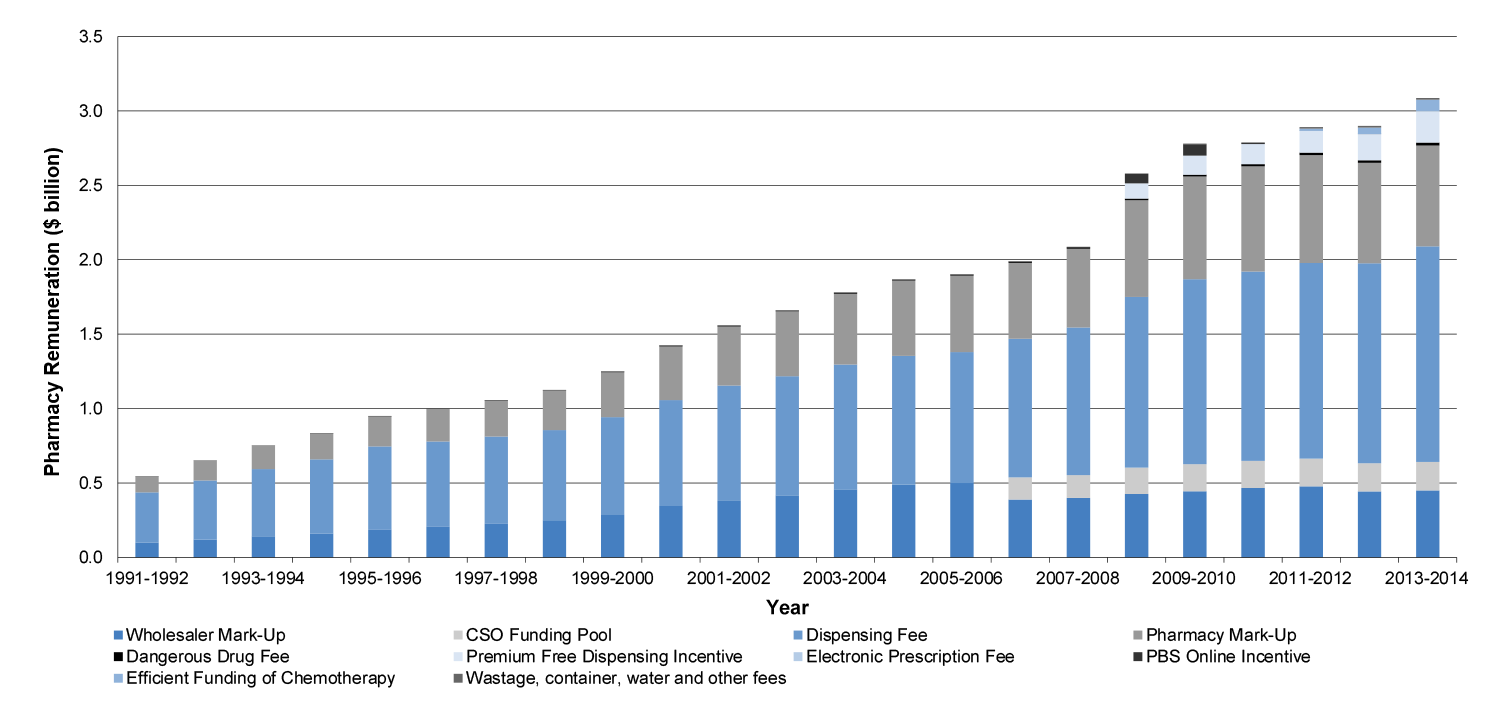
2.26 As outlined in Figure 1.3 and paragraph 1.18, under the 5CPA the specified components of ‘pharmacy remuneration’ are the: wholesale mark-up, pharmacy mark-up, dispensing fee, extemporaneously prepared fee, dangerous drug fee, Premium Free Dispensing Incentive (PFDI) and Electronic Prescription Fee (EPF). The ANAO analysed the total pharmacy remuneration delivered by the 5CPA. About a quarter of PBS and RPBS prescriptions dispensed by retail pharmacies are paid in full by patients—with no Government subsidy—because they are priced under the patient co-payment. However, Health’s estimated $13 771.6 million for 5CPA pharmacy remuneration did not include remuneration received from patients for under co-payment prescriptions.
2.27 On the basis of Health’s advice that the 5CPA (and earlier agreements) included total pharmacy remuneration that it will deliver, this substantial element of remuneration—at least $2.6 billion—could usefully also have been included in the agreement to provide full transparency of total remuneration from the PBS and RPBS. The various sources of pharmacy remuneration are outlined in Figure 2.3.
Figure 2.3: Pharmacy remuneration delivered by the 5CPA—government and patient contributions
Source: ANAO analysis.
Note:
5CPA costs reported in Commonwealth Budget commentary
2.28 The 2010–11 Commonwealth Budget commentary reported the following 5CPA funding, which included the cost of patient co-payments, notwithstanding the reference in the Budget papers to funding provided by the Government:
The Government and the Pharmacy Guild of Australia have signed a new five-year Community Pharmacy Agreement to commence on 1 July 2010 … The agreement will see the Government provide an estimated $15.4 billion over five years from 2010–11 for community pharmacies (including $3.3 billion in 2014-15). This represents an increase of $3.8 billion over the previous agreement, which ends on 30 June 2010.
2.29 There would have been benefit, in the interests of clarifying and clearly documenting the nature of financial commitments entered into by the Australian Government, to explicitly identify the contribution made by the Commonwealth and patients respectively to the $15.4 billion funding commitment in the 5CPA.
2.30 In respect of the statement appearing in the Budget papers, Health advised the ANAO that while the cost of patient co-payments was included in the Budget Paper No. 2 commentary, these costs were not factored into the Budget and forward estimates as a Commonwealth expense:
The PBS forward estimates were only amended to reflect the agreed savings from the various components of the 5CPA. To clarify, the forward estimates were therefore not adjusted by $15.4 billion, but only by the net saving position as a result of the agreed changes from the 4CPA arrangements.
There was only one savings component that incorrectly included patient payments, the Freezing of the Dispensing Fee. As previously agreed with DoFD [Department of Finance and Deregulation], patient payments [co-payments] account for approximately 16% of PBS costs. Therefore of the $267 million save from this measure, only $42.7 million was incorrectly included in the PBS forward estimates. As a percentage of the total PBS forward estimates over that same period this equates to approximately 0.1%.
The reference to the 2010-11 Budget uses the terminology ‘The agreement will see Government provide an estimated $15.4 billion over five years …’ As the agreement is negotiated between the Government and the Guild, although patient contributions are included, the Government is still providing the remuneration arrangements.
2.31 In summary, the 5CPA provides that the Commonwealth ‘will deliver’ funding of $15.4 billion, including some $13.8 billion in pharmacy remuneration. In effect, pharmacy remuneration includes $11.6 billion to be paid by Government and $2.2 billion to be paid by patients. In reporting the estimated costs of the 5CPA—in Health’s advice to Ministers; the written 5CPA agreement; and the 2010–11 Commonwealth Budget commentary—there was no indication that some $2.2 billion of the $15.4 billion in funding would be sourced from patients. Further, while Health considered that the 5CPA should include the total amount that it delivers, additional pharmacy remuneration of at least $2.6 billion for unsubsidised PBS medicines (priced under the patient co-payment and paid by patients) are not mentioned in the 5CPA. To clarify the nature of financial commitments entered into by the Australian Government, the department should present, in key documents, estimated government payments and patient payments for both subsidised and unsubsidised PBS and RPBS medicines.
Recommendation No.1
2.32 To clarify the nature of financial commitments entered into by the Australian Government, the ANAO recommends that the Department of Health presents, in key documents, estimated government payments and patient payments for both subsidised and unsubsidised Pharmaceutical Benefits Scheme and Repatriation Pharmaceutical Benefits Scheme medicines.
Health response: Agreed.
Forecasting the cost of 5CPA dispensing fees
2.33 Dispensing fees are the largest component of pharmacy remuneration under the 5CPA, and the ANAO examined Health’s forecast of dispensing fees in its planning for the agreement. The dispensing fee was indexed annually to Wage Cost Index 9 (WCI9), and WCI9 is documented as the applicable indexation factor for the 5CPA. However, in its 5CPA modelling Health assumed that indexation for the dispensing fee would be 2 per cent per year for the term of the agreement. This indexation rate was significantly higher than the official WCI9 indexation rates as forecast at the time by the Department of Finance and Deregulation (Finance), for use by departments. Applying Finance’s forecast indexation rates would have produced lower dispensing fees under the 5CPA than those forecast by Health, as shown in Table 2.1.
Table 2.1: Comparison of Health’s indexation rates to official forecast
|
Health’s indexation rate:a
|
2.0%
|
2.0%
|
2.0%
|
2.0%
|
2.0%
|
|
Finance’s WCI9 rate:b
|
1.6%
|
1.5%
|
1.6%
|
1.6%
|
-
|
|
Dispensing fees forecast using Health’s indexation rate:
|
$6.55
|
$6.68
|
$6.81
|
$6.95
|
$7.09
|
|
Dispensing fees forecast using official WCI9 rate:
|
$6.52
|
$6.62
|
$6.73
|
$6.83
|
$6.94
|
Source: ANAO analysis of Health and Finance information.
Notes:
2.34 The ANAO estimates that Health’s use of a two per cent indexation rate to forecast dispensing fees, rather than the WCI9 rates released, overestimated the total costs of dispensing fees by some $95 million in the 5CPA baseline.
2.35 In October 2014, Health advised the ANAO that:
Health did not assume an indexation rate. The indexation rate was approved by DoFD [the Department of Finance and Deregulation] as per Budget Operational Rules; the costs were agreed with DoFD prior to 30 March 2010; DoFD was aware of the change to WC19 and then NOT requested a further update to the 5CPA package … while the WCI9 rates available at the time were not used, Finance approved costings using 2%, so clearly they were correct for Finance costing approval processes.
2.36 In late October 2014, Finance advised the ANAO that:
It is clear from the costing models and signed costing agreements that Finance agreed to costings that included the use of a two per cent indexation factor … the costing model prepared by Health and provided to Finance, a copy of which is attached to the signed costing agreement on file states in the ‘Assumptions’ section that: ‘Indexation for the dispensing fee is assumed to be 2% pa.’ It is unclear why a 2 per cent indexation factor was used.
2.37 In summary, Health’s advice provided to Finance on 23 December 2009 indicated that ‘WCI9 (2%)’ was used in Health’s costings. However, the official WCI9 indexation factors released by Finance ranged from 1.5 to 1.6 per cent per year. In advice to the ANAO, Finance confirmed that while it had agreed to Health costings that included the use of a 2 per cent indexation factor, it was unclear from Finance records why this value was used. Finance suggested that one likely explanation was that the relevant Finance officer accepted the information received from Health on face value.
5CPA savings
Budgetary context of 5CPA savings targets
2.38 One of the key objectives of the 5CPA negotiations was to achieve savings to contribute to the structural repair of the Commonwealth Budget. There had been particularly high cost growth under the 4CPA (growth averaged some 9.4 per cent per year) that was due, in part, to a $1.1 billion transitional structural adjustment package (financial assistance) to assist pharmacies adjust to the introduction of Price Disclosure in 2007.
2.39 While Ministers originally proposed a savings target over $1 billion, it was not achieved in the 5CPA negotiations, and consequently the target was reduced. The 5CPA states that:
The initiatives covered by this Agreement result in $1 billion in savings over the Term of the Agreement against the Commonwealth forward estimates.
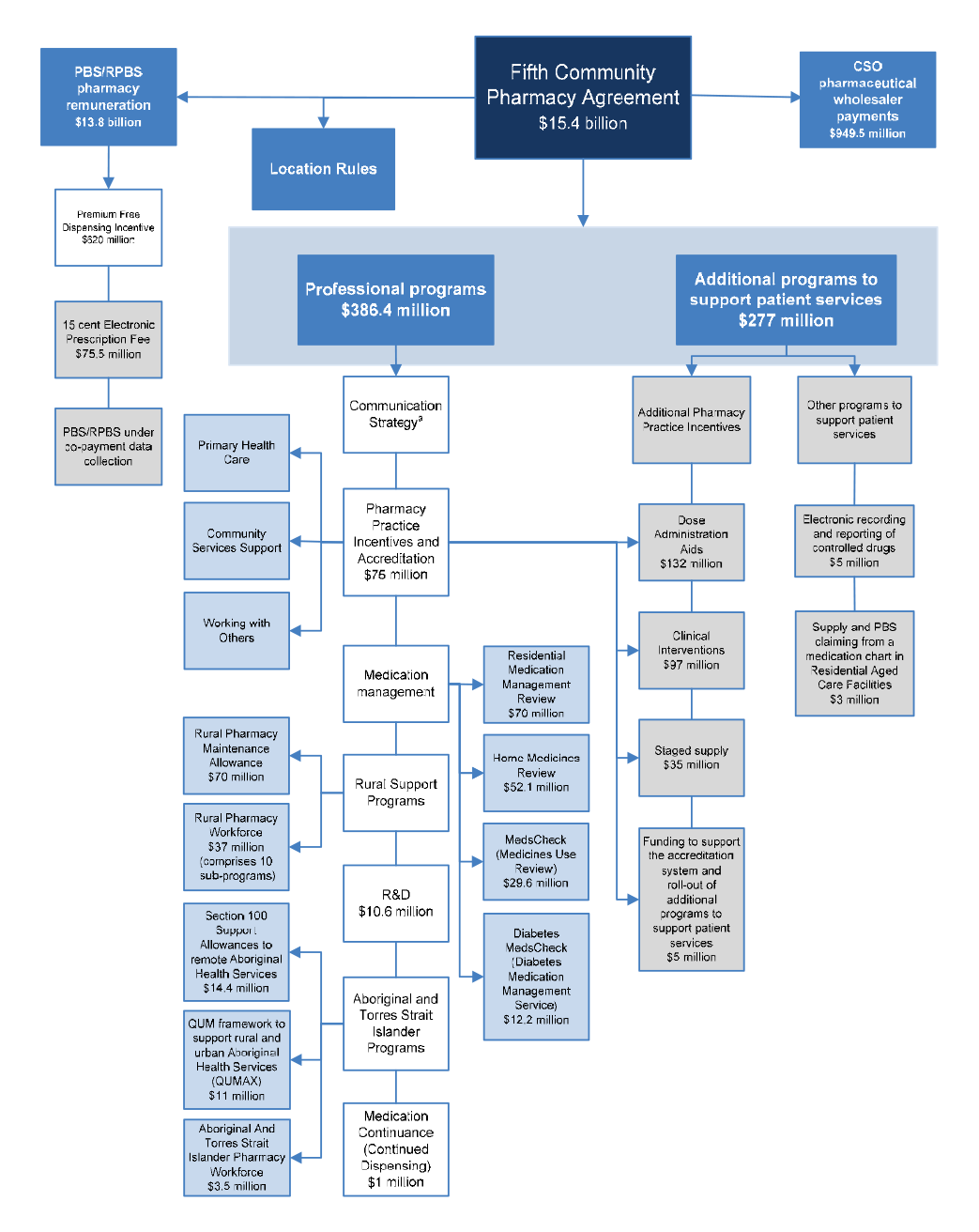
2.40 The 2010–11 Budget Papers clarified that the $1 billion in savings is a gross figure, and after taking into account approved additional expenditure of $0.4 billion, net savings were estimated to be $0.6 billion. The approved additional expenditure of $0.4 billion arises from additional funding of $285.5 million for professional programs and $82.6 million to encourage the electronic processing of prescriptions by pharmacies.
2.41 The 5CPA savings measures discussed in the following paragraphs are: cessation of the PBS Online incentive ($417.7 million); freezing the indexation of the dispensing fee ($267 million) and the CSO Funding Pool ($19.2 million); and reducing funding for professional programs and services ($226.4 million).
Cessation of PBS Online incentive ($417.7 million)
2.42 The largest savings measure negotiated for the 5CPA was the cessation of the PBS Online incentive on 30 June 2010, which Health estimated would deliver $417.7 million in savings.
2.43 The PBS Online incentive was a payment of 40 cents for each prescription that pharmacies claimed through Medicare’s PBS Online system. The incentive was one element of a structural adjustment package that was intended to operate from 1 July 2007 to 30 June 2011. The 40 cent incentive was intended to accelerate pharmacies’ take-up of online claiming. The introduction of the incentive resulted in a rapid and almost complete adoption of PBS Online, with over 97 per cent of pharmacies online by 28 August 2009.
2.44 The departmental estimate of $417.7 million savings from ceasing the PBS Online incentive was based on the assumption that this payment would otherwise continue until 30 June 2015. However, departmental records indicated that the PBS Online incentive was a lapsing measure, and intended to be time limited:
These payments [PBS Online incentive and the Premium Free Dispensing Incentive] were agreed as part of PBS Reform to compensate pharmacy for income they would otherwise lose due to statutory price reductions. The payments were intended to be time limited to provide pharmacy with sufficient time to restructure their businesses as a result of the price reductions. The Government’s commitments to these payments ceases from 1 July 2011 … By 30 June 2011, both incentives will have ensured that the agreed value of the compensation package to pharmacies under PBS Reform has been met.
2.45 Health advised the ANAO that it included the costs of the PBS Online incentive in the last four years of the 5CPA (from 2011–12 to 2014–15) as a saving because the PBS Online incentive was ongoing in the department’s Pharmaceutical Benefit Scheme (PBS) forward estimates.
Dispensing fee indexation freeze ($267 million)
2.46 Under the 4CPA the dispensing fee was indexed annually to Wage Cost Index 9 (WCI9). The second largest savings measure for the 5CPA was the freezing of the dispensing fee at $6.42 for two years, which Health estimated would deliver $267.1 million in savings.
2.47 In examining Health’s costing of the indexation freeze, the ANAO observed that the costing that Health provided to Ministers in April 2010 was not based on the forecast indexation rates that Finance released to agencies in March 2010. Finance’s forecast indexation rates, and those used by Health, are shown in Table 2.1.
2.48 Health advised the ANAO that:
…the WCI9 indexation figures used for the 5CPA costing reflect the agreed indexation amounts from the Department of Finance and Deregulation at the time the costing needed to be finalised, in order to sign the 5CPA by the date requested by Government. This is an issue of timing of the 5CPA needing to be effectively signed off, with figures included, prior to receiving the updated WCI9 figures in March 2010.
2.49 In light of Health’s advice, the ANAO examined the costing agreement between Health and Finance for the dispensing fee freeze, dated 19 January 2010. The forecast WCI9 indexation rates, which were available to Health for the purpose of preparing its costings, had been released by Finance on 17 September 2009. As shown in Table 2.2, the forecast indexation rates released by Finance to agencies in September 2009 differed from the two per cent indexation rate used by Health to cost the dispensing fee freeze.
Table 2.2: Health and Finance forecast indexation rates—September 2009 WCI9
|
Health (January 2010):
|
2.0
|
2.0
|
2.0
|
2.0
|
2.0
|
|
Finance (September 2009):
|
1.6
|
1.6
|
1.5
|
1.6
|
-
|
Source: ANAO analysis of Health and Finance information.
2.50 The ANAO estimated that a consequence of not applying the September 2009 indexation rates released by Finance was that the savings from freezing the dispensing fee were overestimated by approximately $38.7 million for the 5CPA.
2.51 Overall, the estimated saving to government of the proposed dispensing fee freeze under the 5CPA was overestimated by approximately $81.4 million—some 30 per cent of the total saving of $267.1 million—due to the combined effect:
- using higher estimates for indexation than the WCI9 indexation figures provided by Finance (which the ANAO estimates overstated savings by approximately $38.7 million);
- including the patient co-payment in its calculations (which Health advised overstated savings by approximately $42.7 million); and
- using forecast prescription volumes that include public hospital dispensing (which does not attract a dispensing fee).
CSO Funding Pool indexation freeze ($19.2 million)
2.52 The CSO Funding Pool is also indexed by WCI9. Health estimated that savings of $19.2 million would be delivered by not applying indexation to the CSO Funding Pool for the first year of the 5CPA. However, Health again applied a two per cent indexation factor rather than the forecast WCI9 to calculate these savings. The ANAO estimates that Health’s use of incorrect indexation rates overestimated the savings from freezing the CSO Funding Pool by approximately $4.5 million, or some 23 per cent of the total estimated savings of $19.2 million.
2.53 Health advised the ANAO that the CSO costing was approved by Finance at the time. However, as noted previously, while Finance has advised that it agreed to costings prepared by Health which included a two per cent per annum indexation rate across the five years of the 5CPA, this figure did not correspond to Finance’s official WCI9 forecast indexation figures for that period, and there is no documented basis as to why Finance agreed to the change. This experience indicates that there is scope for all entities involved in the planning of the next community pharmacy agreement to document the basis of their costings.
2.54 Further, the repeated application of indexation factors that did not correspond to those released by Finance, indicates that Health should in future exercise care to use the official forecast indexation factors to inform the preparation of its costings.
Recommendation No.2
2.55 To provide assurance regarding the basis of costings for the next community pharmacy agreement, the ANAO recommends that the Department of Health applies the relevant forecast indexation factors released by the Department of Finance.
Health response: Agreed.
Reduced funding for professional programs ($226.4 million)
2.56 The third largest savings measure for the 5CPA was a reduction in funding for professional programs compared to the 4CPA. This measure was reported as delivering $226.4 million in net savings in Budget Paper No. 2, Budget Measures 2010–11.
2.57 Health advised the ANAO that the maximum expenditure on professional programs is capped and the budget is fixed. Accordingly, the baseline cost of professional programs funded under the 5CPA (before being adjusted for any proposed savings or spending measures) should equal the baseline cost of professional programs funded under the 4CPA, adjusted for any authorised ongoing change that may have occurred during the 4CPA. To determine whether this was the case, and whether the intended savings were realised, the ANAO examined Health’s reporting of the baseline costs for 4CPA and 5CPA professional programs, as shown in Table 2.3.
Table 2.3: Comparison of baseline funding for professional programs
|
4CPA budget as reported October 2009
|
168.0a
|
100.0
|
100.0
|
100.0
|
100.0
|
568.0
|
|
5CPA baseline cost adjusted for new funding approved during 4CPA
|
102.7
|
102.2
|
102.2
|
102.2
|
102.2
|
511.6
|
|
5CPA baseline cost as reported October 2009
|
120.0
|
120.0
|
120.0
|
120.0
|
120.0
|
600.0
|
|
5CPA baseline cost as reported April 2010
|
127.7
|
127.7
|
127.7
|
127.7
|
127.7
|
638.7
|
Source: ANAO analysis of Health information.
Note:
2.58 The 4CPA professional program budget was $568 million, which comprised $500 million in 4CPA baseline funding and $68 million that was carried over from the 3CPA. During the 4CPA, the baseline increased by some $2 million per year to fund new programs. In October 2009, Health advised Ministers that the baseline for the 5CPA was $600 million, with no explanation as to why $88.4 million (an additional $17.7 million per year) had been added to the 5CPA baseline. In April 2010, Health further advised Ministers that the 5CPA baseline cost for professional programs was $638.7 million, with no explanation of the further $38.7 million increase.
2.59 In summary, there was an unexplained increase of $127.1 million (comprising $25.4 million per year) in the baseline funding provided by the Government for 5CPA professional programs. Health was unable to provide evidence of Ministerial authority for this significant increase in baseline costs.
Summary of forecast 5CPA savings
2.60 In summary, the ANAO examined the potential savings from the 5CPA savings measures, taking into account the:
- correct values for WCI9 indexation as forecast by Finance at the time Health prepared its costings;
- inclusion of patient co-payments in the savings from freezing the dispensing fee as per Health’s advice to ANAO; and
- unexplained increases in the baseline cost of 5CPA professional programs.
2.61 The ANAO estimates that a more accurate estimate of the net savings from proposed 5CPA measures was approximately $397 million rather than $610 million, as reported in the Budget papers.
Regulatory Impact Statement for the Location Rules
2.62 Health was required to prepare a Regulatory Impact Statement (RIS) as part of its advice to Ministers on the proposed 5CPA because the negotiation of the 5CPA would canvass the regulation of pharmacies through the continued application of the pharmacy Location Rules. The Office of Best Practice Regulation (OBPR) assessed the RIS as inadequate because it did not:
- adequately identify the problem;
- provide an objective assessment of options;
- provide an adequate impact analysis; and
- outline consultation in an adequate manner.
2.63 The OBPR noted that the Location Rules are a restriction on competition, and that the RIS did not demonstrate that the benefits of Location Rules outweighed the costs. Consequently, the OBPR reported the proposal as non-compliant in its 2009–10 Best Practice Regulation Report:
The Department of Health and Ageing (DHA) did not comply in full with the best practice regulation requirements in 2009–10. DHA did not prepare an adequate RIS at the decision-making stage for the proposal to retain pharmacy location rules. DHA is required to commence a post-implementation review of the pharmacy location rules within one to two years of the implementation of the decision.
2.64 In the absence of an adequate RIS, Health was required to undertake a Post Implementation Review (PIR) to examine, among other things, the effectiveness of the regulation in meeting its objectives. According to OBPR guidance, agencies should not require more than three months to complete a PIR. If the regulation is particularly large in scope or in its impacts, then six months may be more adequate. However, the PIR was not finalised until October 2014, over four years after the decision to retain the Location Rules.
2.65 In May 2014, Health advised the ANAO that:
[The] Department did commence the PIR within the two year period as recommended by the OBPR. OBPR did not request the PIR from the Department until September 2012 and the Department provided an initial draft PIR in late 2012. OBPR has since been provided with a further three draft PIRs, incorporating their feedback and responding to their comments. OBPR has also directly assisted with the drafting of the PIR on two occasions. The most recent draft PIR was submitted to OBPR on 8 February 2014. In OBPR’s response to the Department on 14 March 2014 OBPR acknowledged that the PIR largely meets the requirements but that the Government’s regulation requirements had changed since the PIR was drafted and further (additional) information was now required. The Department has been in discussions with OBPR since December 2012 regarding the PIR, with both parties needing to clarify various issues. General agreement has been reached with only some minor amendments to be finalised. It is not accurate to attribute time delays necessarily to the Department.
2.66 On 25 November 2014 the OBPR reported on its website that Health had in October 2014 completed a PIR on the 2010 decision to renew the Location Rules.
Consultation with key stakeholders
2.67 In respect to stakeholder consultation undertaken in developing the 5CPA, Health advised the ANAO that:
From July 2009–January 2010, consultation was undertaken with SHPA [Society of Hospital Pharmacists], UQ [University of Queensland], NPSA [National Pharmaceutical Services Association], PSA [Pharmaceutical Society of Australia], CHF [Consumers Health Forum], Medicines Australia and other stakeholders seeking input and proposals relating to a future Fifth Agreement.
In addition, the CHF was contracted to undertake consumer consultation under a project titled “Fifth Community Pharmacy Agreement Consumer Consultation Project”. The project commenced in January 2010 and findings throughout the consultation were used to inform directions in negotiations. For example the outcomes of the consumer consultation workshop associated with this project were delivered to Health in March 2010.
Consumer consultation
2.68 The department engaged the Consumer Health Forum (CHF) to provide consumer input to the 5CPA in December 2009, and CHF submitted to Health a draft project plan for the proposed community consultation on 12 January 2010. However, the main elements of the 5CPA were agreed in principle on 24 December 2009, through an exchange of letters between the Minister for Health and the Pharmacy Guild.
2.69 The CHF consulted widely with consumer representatives through teleconferences, a national workshop and meetings, in accordance with the project plan approved by Health. While participants in the national workshop provided useful information from a health consumers’ perspective, a number expressed concern that consumer input would not have significant impact on the 5CPA, given that it had already been agreed in principle. The CHF submitted its final report to Health on 27 May 2010, some 24 days after the 5CPA was signed by the Health Minister and Pharmacy Guild on 3 May 2010.
2.70 The CHF advised the ANAO that:
Following CHF’s submission of contract reports [to Health], there was limited discussion of the 5CPA. CHF undertook (in collaboration with a number of other pharmacy and health groups including the Society of Hospital Pharmacists, APESMA [now Professional Pharmacists Australia] and the Public Health Association) to initiate a senate inquiry into the Community Pharmacy Agreements (CPAs), which was unsuccessful. We also jointly wrote to the [then] Minister conveying our concerns about the lack of consultation with consumer and pharmacy groups at the negotiation stage of the Agreements. The Minister referred this correspondence to the Department, which then conducted two meetings with these groups in late 2010 … The discussions centred on the extent to which these groups were excluded from discussions on CPAs and a place at the table for discussions on the 6CPA. There has been ongoing criticism in the pharmacy press about the lack of consultation on the 6CPA and it seems very little has changed in the approach that the Department takes to these arrangements. As a consumer organisation, these arrangements seemed highly inappropriate and out of step with requirements for transparency and accountability of government agreements, particularly those involving billions of taxpayer dollars.
Consultations with professional organisations
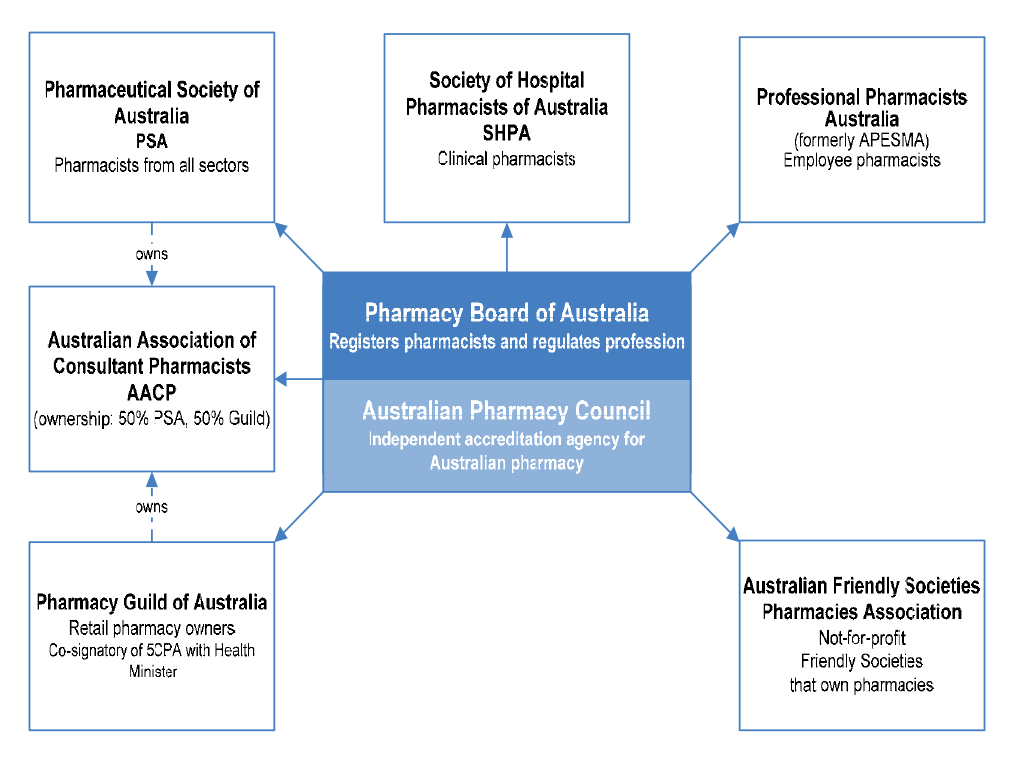
2.71 Although the Pharmaceutical Society of Australia (PSA) is not a signatory to the 5CPA, it is the largest professional association of pharmacists in Australia, and its role is recognised in the 5CPA as follows:
The parties understand that the Pharmaceutical Society of Australia, whilst not a signatory to this Agreement, will be an active participant in those areas of this Agreement that are related to professional practice.
2.72 A peak pharmacists body advised the ANAO that in respect to the development and negotiation of the 5CPA, it considers that:
There is little transparency … For example, this lack of transparency was evident in the secrecy surrounding the development of initial proposals that were subsequently negotiated between the Guild and DoHA [Health]. The outcome of these secret negotiations was announced on Christmas Eve 2009 by the then Minister for Health and Ageing as the ‘major components’ of an agreed 5CPA with funding of $15.1 billion (at that time). After several representations, [this body] was offered a belated opportunity to present proposals to the Department and the Guild for consideration for inclusion in 5CPA and during early 2010 [this body] drafted proposals and provided the evidence-bases for a Clinical Interventions program and a Medicines Use Review program. At its own expense, [this body] also ensured that experts were made available to DoHA to discuss more detailed aspects of the Clinical Interventions program. [This body] also made its views known that the funding allocated to some individual 5CPA programs (such as Home Medicine Reviews) was inadequate.
2.73 Other peak bodies that made submissions to the ANAO regarding the 5CPA also expressed concerns that the processes for developing and negotiating the 5CPA did not provide an opportunity for effective engagement prior to it being finalised.
Negotiations with the Pharmacy Guild
Negotiation process and record keeping
2.74 Health’s negotiating team consisted of three departmental executives, and several support staff. The head of the negotiation team advised the ANAO that there was extensive engagement with Health’s senior executive throughout the negotiations.
2.75 Health advised the ANAO that the negotiations involved ‘dozens of meetings’ with the Pharmacy Guild, which were conducted face to face, by email, telephone and teleconference. However, Health also advised that it had not kept a formal record of its meetings and discussions with the Pharmacy Guild. Health advised the ANAO that for the duration of the negotiations, it did not:
- keep a record of its meetings with the Pharmacy Guild;
- take minutes of meetings; or
- prepare agreed notes of what had been discussed.
2.76 Given the significance of the issues under negotiation, the decision not to prepare an official record of discussions was not consistent with sound practice and potentially limits the department’s capacity to satisfy accountability requirements and protect the Commonwealth’s interests. Appropriate record keeping enables government entities to discharge accountability and advisory obligations to Government and the Parliament, and to contribute effectively to audit, FOI and administrative review processes. It also enables departments to protect the Commonwealth’s interests in the event of disputes and legal action.
2.77 The department should maintain an adequate record of the negotiation of the next community pharmacy agreement. In view of the approach to record keeping adopted in negotiating the 5CPA, Health should also review its internal guidance on appropriate record keeping practices relating to the negotiation of significant contracts and agreements.
Recommendation No.3
2.78 To improve its ability to satisfy accountability requirements and capacity to protect the interests of the Commonwealth in the event of disputes or legal action, the ANAO recommends that the Department of Health:
- maintains an adequate record of the negotiation of the next community pharmacy agreement and related contracts; and
- reviews its internal guidance on record keeping for the negotiation of significant contracts and agreements.
Health response: Agreed.
Risk management
2.79 Systematic risk management practices enable entities to be confident that implementation has been designed to achieve government objectives most effectively.
2.80 Notwithstanding the complexity and high value of the agreement, Health records indicate that in its preparations for the 5CPA negotiations and implementation, the department did not: develop a risk management plan; develop a probity plan or consult with a probity advisor; complete specific conflict of interest declarations for members of its negotiation team; or develop a strategic implementation plan.
2.81 Health advised the ANAO that:
No written risk management plan specifically for 5CPA negotiations [was] prepared; however, the risks associated with the negotiations were actively managed through regular communication with the Departmental Executive and Minister’s Office. Risk management actions were undertaken before and during the negotiation process, such as consultation with a range of interested parties to ensure their views were considered. In addition, the CHF were separately contracted to provide advice on the consumer perspectives for the negotiation and implementation.
2.82 Health advised the ANAO that the negotiation team sought legal advice on issues ‘as required’—arranged through the department’s Legal Services Branch—but not regarding probity issues.
2.83 In respect of the management of potential conflicts of interest, Health advised the ANAO that it relied on routine declaration of interest processes for its staff involved in the negotiations, rather than solicit declarations specifically for the negotiation process.
2.84 Health advised the ANAO that a framework has been put in place to record key decisions made in the course of negotiations for a future agreement.
Government objectives in the 5CPA negotiations
2.85 Ministers set nine objectives for negotiating the 5CPA, including a savings target over five years of significantly more than $1 billion.,
2.86 The then Government and department also considered that the 5CPA offered an opportunity to improve health outcomes and value for money by restructuring pharmacy remuneration arrangements ‘to diminish their link to the price of PBS medicines’. The Commonwealth anticipated doing so by shifting financial incentives from the volume driven sale of medicines to the delivery of value-adding professional services.
2.87 Some of the other negotiating objectives for the 5CPA included:
- better quality care and patient access to care in pharmacies and other health care settings, by investing in more effective and cost-effective health services provided by pharmacies and pharmacists;
- reformed programs that focus on improving medication-related services to patients;
- support for information technology systems that leverage investment from the pharmacy sector and are fully interoperable with broader e-health systems, including current and prospective National eHealth Transition Authority standards;
- access to the full range of PBS data, including prescriptions that cost less than the general patient co-payment—considered to be a ‘non-negotiable’ objective—which would help the Commonwealth determine actual PBS pharmacy remuneration from all sources, including patients, and the total volume and cost of the PBS to both government and consumers; and
- appropriate remuneration for pharmacies for chemotherapy infusions.
Revised 5CPA negotiation objectives
2.88 On 14 December 2009, Health provided an update on the 5CPA negotiations to Ministers. Health advised that the Pharmacy Guild had identified some $1 billion in potential savings, including savings from private hospital pharmacy and the Safety Net, but opposed changes to the structure of pharmacy remuneration. In addition, the Guild sought to retain the transitional 4CPA structural adjustment package that was due to expire on 30 June 2011.
2.89 While the Pharmacy Guild had identified some $1 billion in potential savings, it also sought additional funding of: $277 million in compensation for the effects of revised Price Disclosure arrangements; and $75.5 million for the processing of electronic prescriptions and funding for software vendors, to integrate a range of agreement–related elements into existing dispensing software for pharmacies.
2.90 Ministers agreed that the Health Minister should pursue savings over five years relating to both the 5CPA and revised Price Disclosure arrangements, but would not offer compensation for the flow-on effects of the revised Price Disclosure arrangements. However, Ministers did agree to consider some additional payments to pharmacies for delivering improved professional health services.
2.91 Ministers also agreed that the Health Minister develop a revised negotiating package incorporating the Government’s position and taking into account the Pharmacy Guild’s offer. If further negotiations were successful, the Health Minister would write to seek Ministers’ agreement to the final negotiated package, with costs to be agreed by Finance before exchanging a Letter of Intent with the Pharmacy Guild.
2.92 On 23 December 2009, Health advised the Health Minister that the proposed 5CPA would deliver $1 billion in gross savings, and that costings for the savings were currently being agreed with Finance. On that basis, Health recommended that the Health Minister sign the Letter of Intent with the Pharmacy Guild, which the Minister signed on 24 December 2009.
2.93 The ANAO requested that Health provide documentation of relevant Finance approvals and correspondence seeking Ministers’ agreement to the final negotiated package before the Letter of Intent was exchanged with the Pharmacy Guild. Health advised the ANAO that relevant documentation did not exist. The department further advised, in February 2015, that:
the core issue is that no formal written advice directing the Department to proceed with the associated Minute and Letter of Intent exists. While authority was given verbally, the Department acknowledges that better practice would have been to record this in a file note. However, any implication that the Department acted without Government knowledge or authority is incorrect.
The Report has only considered the Department’s advice that such a request was made, and that the Minister was satisfied in exercising their decision by virtue of signing the Letter of Intent. The Department accepts that in future, formal written advice should be obtained for record-keeping purposes to ensure an audit trail of any requests made can be furnished.
As evidenced by records considered by the Report, the Fifth Agreement negotiations were dynamic and often compressed in order to meet required timeframes. The Department remains of the view that in all instances it sought to be responsive to Government priorities and objectives. The above is an example of an area for improvement in the future and accordingly, the Department maintains its agreement to Recommendations 3 and 5 in the proposed Report that relate to record-keeping.
2.94 In the absence of Health documentation, the ANAO also examined Finance records relating to the 5CPA. Finance records indicate that while various 5CPA savings measures were agreed by Finance between 13 January 2010 and 7 April 2010, none were agreed prior to the signing of the Letter of Intent on 24 December 2009, and some were agreed over three months afterwards. The largest savings measure—cessation of the PBS Online Incentive payment ($417.7 million)—was not agreed by Finance until 1 April 2010. Finance provided its first assessment of the cessation of the PBS Online incentive to Health in a facsimile dated 12 March 2010. In that message, Finance indicated that it had not provided input on costs for this savings measure:
This costing relates to a proposal agreed by SPBC [Strategic Priorities Budget Committee] on 14 December 2009 as part of the 5CPA. Agreeing to costs post a decision by SPBC is a deviation from usual process where costs are agreed by Finance prior to the proposal being considered for decisions by SPBC (or ERC) [Expenditure Review Committee]. The SPBC decision accepted this savings proposal and provided authority to the Minister for Health and Ageing to use it as part of their negotiations, hence, Finance has no input in relation to the policy.
2.95 It is not uncommon for Ministers, in the context of government decision-making processes, to request additional follow-up action, and it is incumbent on departments to implement appropriate systems to ensure that such requests are actioned. The ANAO has recently commented on other instances where departments have failed to do so, and there would be benefit in Health reviewing its internal processes relating to the implementation of action requested by Ministers through Cabinet processes.
Outcome of negotiations
2.96 Ministers noted the outcome of the 5CPA negotiations on 9 April 2010 and agreed to the savings measures and funding arrangements proposed for the agreement, including estimated savings to government of $1 billion, and new spending measures of $0.4 billion. The largest new spending measures were: $269 million for pharmacies that registered for Pharmacy Practice Incentives, which required accreditation with the Pharmacy Guild’s Quality Care Pharmacy Program (QCPP); and $75.5 million for an Electronic Prescription Fee for pharmacies to offset the cost of downloading electronic prescriptions from a Prescription Exchange Service. The 5CPA was signed on 3 May 2010 by the Health Minister and the Pharmacy Guild.
2.97 A number of the Commonwealth’s strategic negotiating objectives for the 5CPA were only partially realised. Although the net forecast savings to Government were approximately $0.6 billion, due to shortcomings in Health’s costing methodology, the expected savings were more likely to be approximately $0.4 billion.
2.98 The Government considered that the 5CPA offered an opportunity to improve health outcomes and value for money by restructuring pharmacy remuneration arrangements ‘to diminish their link to the price of PBS medicines’. The Commonwealth anticipated doing so by shifting financial incentives from the volume driven sale of medicines to the delivery of value-adding professional services. However, the structure of pharmacy remuneration remained essentially unchanged from the 4CPA to the 5CPA—based on defined mark-ups to the base price of pharmaceuticals and the addition of a variety of fees. Further, key wholesaler and pharmacy mark-ups continued at previous rates.
2.99 A further Commonwealth negotiating objective, which Ministers considered to be ‘non-negotiable’, related to obtaining access from pharmacies to the full range of PBS data, including information relating to prescriptions that cost less than the general patient co-payment. As discussed, this information would help the Commonwealth determine actual PBS pharmacy remuneration from all sources, including patients, and the total volume and cost of the PBS to both government and consumers. This objective was partially realised—while the 5CPA made provision for pharmacies to provide certain prescription information from 1 April 2012, it did not make provision for the receipt of cost information.
2.100 A key negotiating objective of the 5CPA was to implement more appropriate pharmacy remuneration for chemotherapy infusions. However, the negotiation outcome required additional consideration and government funding some 18 months after the 5CPA was signed.
2.101 Another key negotiating objective of the 5CPA was to support information technology systems that are fully interoperable with broader e-health systems. However, the two Prescription Exchange Services (PESs) that were approved by Health for the purpose of downloading electronic prescriptions by pharmacies, did not have systems that were interoperable. Government funding for the Electronic Prescription Fee was subsequently re-allocated to pay the PESs directly to make their systems interoperable.
2.102 In respect of the ‘non-negotiable’ Commonwealth objectives that were not met, Health advised the ANAO in February 2015 that:
in any negotiation, objectives may or may not be fully realised for a variety of factors. While it is therefore correct that not all the negotiating objectives agreed by Government prior to the commencement of the negotiations were met—it is reasonable to assert that nonetheless, Government was satisfied sufficient objectives were realised through their agreement to the final package of measures at the conclusion of negotiations, as approved by the Cabinet.
Pharmacy Guild contracts
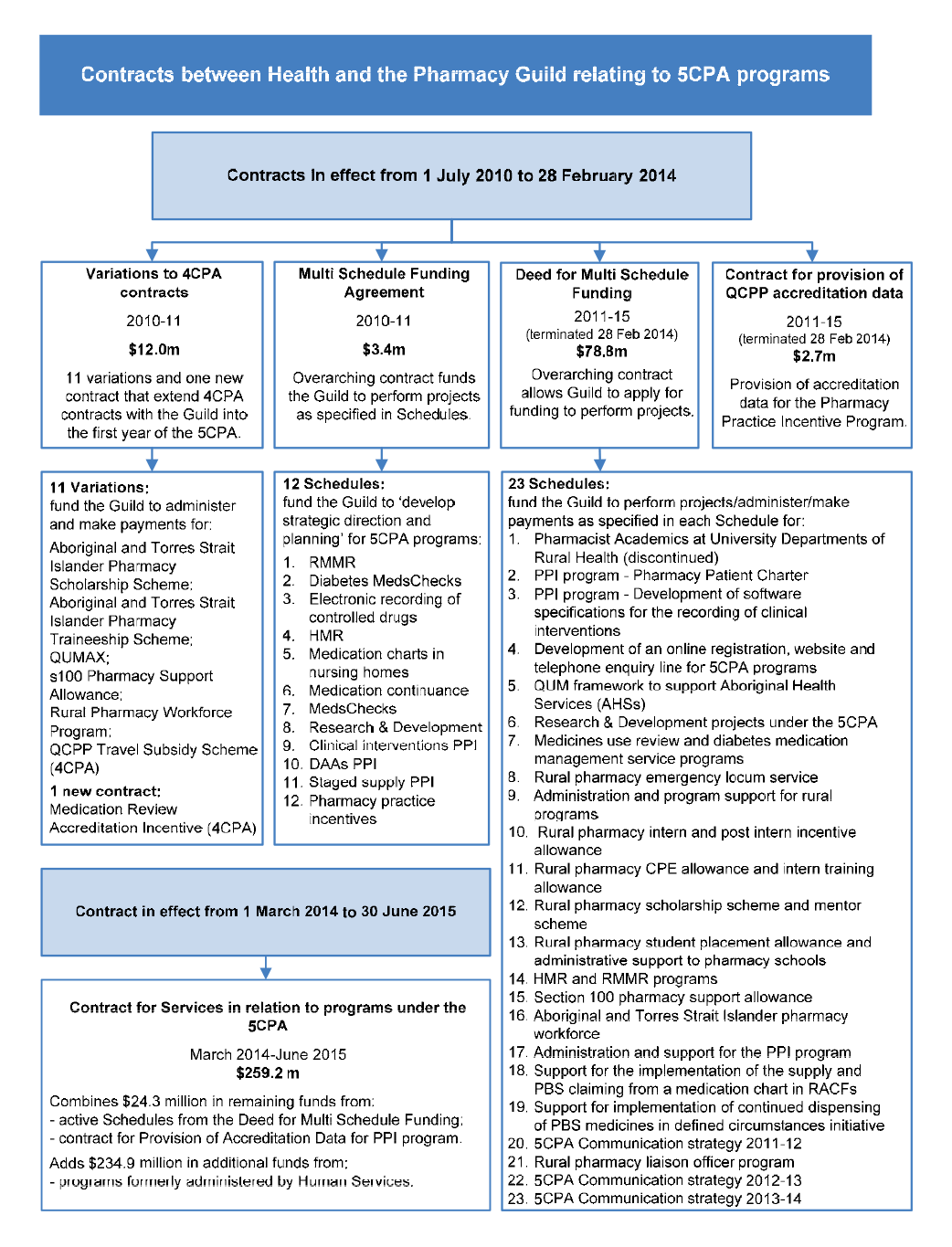
2.103 After the 5CPA was signed, Health entered into a range of contracts with the Pharmacy Guild relating to the agreement. These included:
- a Multi Schedule Funding Agreement with twelve Schedules that provided a total of $3.4 million in funding to the Guild to ‘develop strategic direction and planning’ for 5CPA programs;
- a Deed for Multi Schedule Funding with 23 Schedules that provided a total of $79 million funding to the Guild to make program payments and provide administrative services;
- a contract that provided $2.7 million to the Guild to provide accreditation data for the Pharmacy Practice Incentives program; and
- variations to 4CPA contracts that provided $12 million to the Guild to continue making program payments and administering 4CPA programs in the first year of the 5CPA.
2.104 Health also entered into eight contracts with a Pharmacy Guild related entity known as Fred IT Group, to provide funding of up to $22.9 million. Two of these eight contracts are for services relating to the 5CPA.
2.105 In common with the approach adopted for the earlier 5CPA negotiations, Health did not document its discussions and negotiations with the Pharmacy Guild relating to the negotiation of the contracts.
Conclusion
2.106 The department developed and negotiated a complex agreement and related contracts with the Pharmacy Guild in a timely manner, enabling the 5CPA to be signed by the Health Minister and the Guild on 3 May 2010, prior to the expiry of the 4CPA on 30 June 2010. However, a number of key government negotiating objectives for the 5CPA were only partially realised and there were shortcomings in key aspects of Health’s administration at the development and negotiation phases.
2.107 Health advised that its planning for the 5CPA involved reviewing evaluations of components of the 4CPA. One evaluation was completed before the 5CPA was signed and eleven were completed afterwards.
2.108 The 5CPA committed the Commonwealth to delivering funding of $15.4 billion—including $13.8 billion in pharmacy remuneration for PBS and RPBS dispensing, comprising $11.6 billion to be paid by Government and $2.2 billion to be paid by patients. In reporting the estimated costs of the 5CPA—in Health’s advice to Ministers; the written 5CPA agreement; and the 2010–11 Commonwealth Budget commentary—there was no indication that some $2.2 billion of the $15.4 billion in funding would be sourced from patients. Further, while Health considered that the 5CPA should include the total amount that it delivers, additional pharmacy remuneration of at least $2.6 billion for unsubsidised PBS medicines (priced under the patient co-payment and paid by patients) are not mentioned in the 5CPA. To clarify the nature of financial commitments entered into by the Australian Government, the department should present, in key documents, estimated government payments and patient payments for both subsidised and unsubsidised PBS and RPBS medicines.
2.109 Clause 1.2(e) of the 5CPA provides that: ‘The initiatives covered by this Agreement result in $1 billion in savings over the Term of the Agreement against the Commonwealth forward estimates.’ The 2010-11 Budget Papers clarified that the $1 billion in savings is a gross figure, and after taking into account approved additional expenditure of $0.4 billion, net savings were estimated to be $0.6 billion. The difference of $0.4 billion results from additional funding of $285.5 million for professional programs and $82.6 million to encourage the downloading of electronic prescriptions by pharmacies.
2.110 ANAO analysis indicates that the net savings estimated before the agreement was signed were closer to $0.4 billion (rather than $0.6 billion) due to shortcomings in the department’s 5CPA estimation methodology. The principal issues relate to: unexplained increases in the baseline cost of professional programs; the application of inappropriate indexation factors; and the treatment of patient co-payments. In particular:
- The baseline budget for 5CPA professional programs in the Commonwealth forward estimates was $638.7 million (before adjusting for the negotiated 5CPA savings and spending measures). However, Health’s records showed that the approved 5CPA baseline budget for professional programs was only $511.6 million, and there was no documentary evidence of authority to increase the 5CPA baseline budget in the forward estimates by $127.1 million.
- The official indexation factors released by the then Department of Finance and Deregulation (Finance) were not utilised in estimating 5CPA savings, resulting in an overestimate of 5CPA savings of approximately $43.2 million. The repeated application of indexation factors that did not correspond to those released by Finance, indicates that Health should in future exercise care to use the official forecast indexation factors to inform the preparation of its costings.
- Health advised, in the course of this audit, that the estimated savings for the 5CPA incorrectly included $42.7 million in co-payments made by patients to pharmacies for the receipt of pharmaceutical benefits. Co-payments are a private contribution to the cost of PBS medicines, which are not a cost to government.
2.111 In addition to the shortfall in anticipated savings, a number of the Commonwealth’s other strategic negotiating objectives for the 5CPA were only partially realised. In particular:
- The then Government and department considered that the 5CPA offered an opportunity to improve health outcomes and value for money by restructuring pharmacy remuneration arrangements ‘to diminish their link to the price of PBS medicines’. The Commonwealth anticipated doing so by shifting financial incentives from the volume driven sale of medicines to the delivery of value-adding professional services. However, the structure of pharmacy remuneration remained essentially unchanged from the 4CPA to the 5CPA—based on defined mark-ups to the base price of pharmaceuticals and the addition of a variety of fees. Further, key wholesaler and pharmacy mark-ups continued at previous rates.
- A negotiating objective which Ministers considered to be ‘non-negotiable’, related to obtaining access from pharmacies to the full range of PBS data, including information relating to prescriptions that cost less than the general patient co-payment. This information would help the Commonwealth determine actual PBS pharmacy remuneration from all sources, including patients, and the total volume and cost of the PBS to both government and consumers. This objective was partially realised—while the 5CPA made provision for pharmacies to provide certain prescription information from 1 April 2012, it did not make provision for the receipt of cost information.
- The Government wished to support information technology systems that were fully interoperable with broader e-health systems. However, the two Prescription Exchange Services (PESs) that were approved by Health for the purpose of downloading electronic prescriptions by pharmacies, did not have systems that were interoperable. As discussed in Chapter 3, Government funding for the Electronic Prescription Fee (EPF) was subsequently re-allocated to pay the PESs directly to make their systems interoperable.
- The Government also wished to implement more appropriate pharmacy remuneration for chemotherapy infusions, with any additional funding to be settled within the 5CPA funding envelope. However, the negotiation outcome for chemotherapy remuneration required additional consideration and a further $82 million in government funding some 18 months after the 5CPA was signed.
2.112 The ANAO identified persistent shortcomings in departmental record-keeping relating to the 5CPA. In December 2009, Ministers had agreed that the Health Minister would write to seek the agreement of Ministers to the final 5CPA negotiated package, with costs agreed by Finance, before exchanging a Letter of Intent with the Pharmacy Guild. The ANAO requested that Health provide documentation of relevant Finance approvals and correspondence seeking the agreement of Ministers to the final package negotiated with the Pharmacy Guild. Health advised the ANAO that relevant documentation did not exist.
2.113 Health recommended that the Health Minister sign the Letter of Intent with the Pharmacy Guild on the basis that costings for the savings were currently being agreed with Finance, and the Minister signed the Letter of Intent on 24 December 2009. Department of Finance records indicate that while various 5CPA savings measures were agreed by Finance between 13 January 2010 and 7 April 2010, none were agreed prior to the signing of the Letter of Intent in December 2009, and some were agreed over three months afterwards.
2.114 The department also advised the ANAO that during the 5CPA negotiations, it did not keep a formal record of its meetings with the Pharmacy Guild and did not document its subsequent discussions with the Guild on the negotiation of contracts relating to the 5CPA. Given the significance of the issues under negotiation, the decision not to prepare an official record of discussions was not consistent with sound practice, as shortcomings in record keeping can affect a government entity’s capacity to discharge advisory, accountability and contract management obligations. The department should maintain an adequate record of the negotiation of the next community pharmacy agreement. In view of the approach to record keeping adopted in negotiating the 5CPA, Health should also review its internal guidance on appropriate record keeping practices relating to the negotiation of significant contracts and agreements.
2.115 Notwithstanding the complexity and high value of the agreement, Health records indicate that in its preparations for the 5CPA negotiations and implementation, the department did not: develop a risk management plan; develop a probity plan or consult with a probity advisor; complete specific conflict of interest declarations for members of its negotiation team; or develop a strategic implementation plan.