Browse our range of reports and publications including performance and financial statement audit reports, assurance review reports, information reports and annual reports.
Auditor-General Report No. 25 of 2007–08
Administering Round the Clock Medicare Grants
Published
Wednesday 27 February 2008
Portfolio
Health and Ageing
Entity
Department of Health and Ageing
Sector
Ageing
Health
The objective of the audit was to examine the effectiveness of the Department of Health and Ageing's administration of the Round the Clock Medicare: Investing in After Hours General Practice Services program.
Summary
Introduction
After hours general practice in Australia
Primary care is an essential component of the health system through which Australians access a range of diagnostic, pharmaceutical and acute health care services. The ability to access a general practitioner (GP) after hours is an important element of primary care.1 Over the period 2001–02 to 2005–06, there was a nine per cent decrease (from 56 per cent to 47 per cent) in the proportion of GPs providing after hours primary care. The capacity of GPs to meet after hours service demands has been linked to, among others things, the current GP workforce shortage.
The Australian Government has implemented a number of programs to address the need for after hours GP services. Administered by the Department of Health and Ageing (DoHA) or Medicare Australia, these initiatives include: Round the Clock Medicare (RTCM); After Hours Primary Medical Care Program; Practice Incentives Program; and the National Health Call Centre Network.
Round the Clock Medicare: Investing in After Hours General Practice Services
RTCM was announced as part of the Coalition Government's 2004 election policy and commenced in 2005. RTCM has two components—RTCM: Higher Rebates for After Hours General Practice Services and RTCM: Investing in After Hours General Practice Services. This audit report focuses on the grants aspect of RTCM, that is, Investing in After Hours General Practice Services. Administered by DoHA, Investing in After Hours General Practice Services aims to ‘improve after hours GP access in metropolitan and regional Australia'.2
For the period 2004–05 to 2008–09, RTCM: Investing in After Hours General Practice Services has a total budget of $62.5 million. This amount funds three different components:
- supplementary grants—provide up to $50 000 for two years, to assist after hours services to meet their marginal costs;
- operating subsidies—are worth a maximum of $200 000 per year for up to three years. They are used to support new or recently established well located after hours clinics and Medical Deputising Services (MDS) establishing clinic based after hours services;
- start-up grants—provide up to $200 000 over two years. They are used to assist existing general practices and dedicated after hours clinics to remain open and mobile MDSs wishing to establish clinic based after hours services.
The 2004 Coalition election policy identified five sites to receive 2004–05 start–up grants. The full program commenced in 2005–06, with three competitive grants rounds completed and a fourth expected in 2008–09. To October 2007, DoHA had executed 144 funding agreements, with a further 85 under negotiation, as shown in the following figure.
Figure 1 Number of funding agreements, as at October 2007
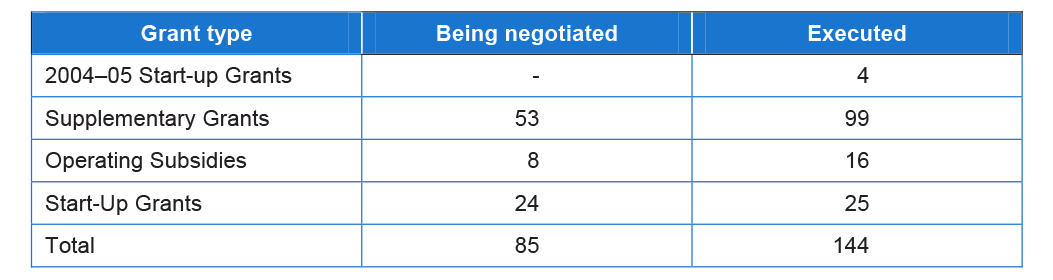
Source: ANAO analysis of DoHA data.
Figure 2 provides a brief overview of DoHA's administration of the program.
Figure 2 Overview of the program
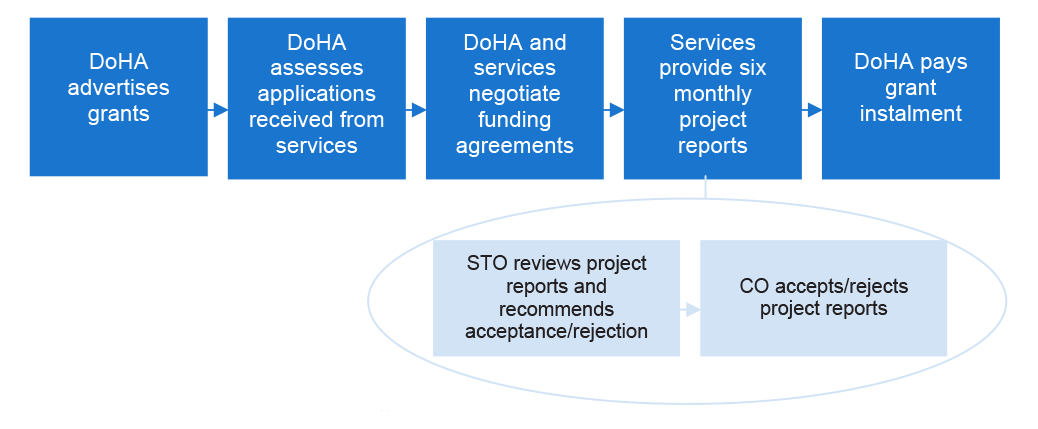
Note: STO - DoHA's State and Territory Offices
CO = DoHA's Central Office
Source: ANAO analysis
Audit scope and objectives
The objective of the audit was:
to examine the effectiveness of DoHA's administration of the Round the Clock Medicare: Investing in After Hours General Practice Services program.
The audit focused on the grants aspect of RTCM—Round the Clock Medicare: Investing in After Hours General Practice Services. The audit did not include an examination of DoHA's role in providing Medicare rebates to after hours GP services.
Audit conclusion
In 2004–05, DoHA responded to the Coalition Government's decision to introduce RTCM, rapidly implementing the grants program. The aim of the RTCM grants program is to provide greater incentives for GPs to practice after hours and to invest in after hours GP infrastructure. The Coalition Government's intention was to target the funding of services in areas of high demand, such as outer metropolitan, regional and remote areas.
To administer RTCM, DoHA developed functional program documents, including application forms and guidelines for applicants, and a process for assessing grant applications. Following the 2004–05 funding round, DoHA reviewed and reissued its program guidance and application forms and established procedures to assess grant applications and negotiate funding agreements in a timely manner. GP services are generally supportive of DoHA's processes and report a good working relationship with the Department.
The grants program has been established for three years and, as such, it is now timely for DoHA to consolidate and build on the lessons learned. DoHA's administration of RTCM could be strengthened by improvements at the operational level and by evaluating the extent to which the program is meeting its objectives.
At the operational level, DoHA could better target its assessment of project performance reports to obtain adequate assurance about the accuracy of data provided by grant recipients. Grant recipients supply these data to illustrate progress and compliance with the conditions of their funding agreements. To ensure program integrity, it is important that DoHA establish a cost-effective risk-based system to verify data provided by funded services.
In addition, evaluating RTCM would assist DoHA to determine whether it is succeeding in its aim to provide greater incentives for GPs to practice after hours and to invest in after hours GP infrastructure and, consequently, to understand how the program is impacting on the provision of after hours GP services in Australia. While DoHA recognises the need to evaluate RTCM, it does not have a current plan to do so. Accordingly, after three years, DoHA has little analysis to inform decisions about any possible changes that may improve the services provided.
For DoHA to be in a position to determine whether the program is meeting its aims, it also needs to develop and make use of a more effective performance management framework. The RTCM performance indicator is a single broad measure of performance that assesses the number of services funded. It does not capture other key elements of the objectives of the program, particularly the provision of services to areas of high demand. Measuring and reporting the number of services funded does not inform DoHA, Parliament, or the Australian public, about where, when or how these services are being provided, the quality of the service, the patients being treated, or the workforce providing the services. Nor does the indicator assist DoHA's program managers to administer the program.
The ANAO has made a number of suggestions and three recommendations to DoHA that will assist it to improve its administration of RTCM. DoHA agreed to all three recommendations.
Key findings
Design and Planning
Establishing the RTCM framework
RTCM's program documents state that priority for funding will be given to services in outer suburban, regional and remote areas of Australia. The early planning phase of the program explored options on how to prioritise areas of need. However, none of these options had been implemented. Furthermore, the grant promotion and written assessment processes do not have a mechanism to allow for priority to be given to outer suburban, regional or remote areas.
The Program Guidelines state that services should aim to become self sustainable within the grant funding period. DoHA recognises that, for some services to remain viable, they may require longer term financial support. Nevertheless, sustainability of funded after-hour GP services is a goal of RTCM. However, sustainability has not been built into many of the services' models receiving grants. Without ongoing Government support, these services may be unsustainable in the long term.
Performance management
DoHA has not established an effective performance management framework for RTCM. A single performance indicator for the program is outlined in DoHA's Portfolio Budget Statements and measures the program's progress by the number of services funded. However, there is no link between this high level performance indicator and other key elements of the program, particularly the provision of services to areas of high demand.
At an operational level, DoHA monitors services' progress and compliance with funding agreements through a six-monthly reporting system. However, the focus of the reporting system is the progress of individual services. DoHA's monitoring and analysis does not include an examination of trends across time or progress within and across grant types, across regions, or across the program as a whole.
DoHA has not established a performance baseline for the program or its individual funding components. Prior to the introduction of RTCM Medicare Benefits Schedule (MBS) items, Medicare items did not provide DoHA with sufficient information to determine the extent of existing after hours GP coverage. Without this baseline information it will be difficult for DoHA to measure the success of the program and ascertain the extent to which the grant categories are meeting their objectives.
Key definitions
Terms such as ‘after hours' and ‘access' are not clearly articulated in DoHA's program documentation. Additionally, the definition of ‘after hours' in RTCM differs from that used in other government initiatives. When evaluating RTCM, DoHA should consider the benefits and costs of employing a clear and consistent definition of after hours across all of its programs.
Evaluating the program
DoHA has not evaluated RTCM and it is currently drafting an evaluation plan. Although DoHA had developed a draft evaluation framework in early 2005, it was unable to provide the ANAO with any later reference to the framework. Without implementing a strategy to evaluate RTCM, DoHA will find it difficult to determine whether the program's objectives are being achieved.
Assessing and Allocating Grants
Guidance for DoHA personnel
Clear, consistent and well-documented guidance material is an important component of an efficient and effective grants program. DoHA personnel from both Central Office (CO) and State and Territory Offices (STOs) undertake their roles and responsibilities with the support of a variety of guidance materials. These include the Project Manager's Toolkit, the Program Guidelines and the Program Management Guide. Staff also have access to specialist areas within DoHA, such as the Legal Services Branch (LSB) and the Primary and Ambulatory Care Division's Contract Management Advisory Unit (CMAU). However, DoHA has not developed a central program management guide for its staff. Such a guide, regularly updated, would assist consistency in decision making and efficient administration of the program.
Assessing grant applications
DoHA has established an appropriate process to assess grant applications. The Department has also produced relevant documentation to support this process. DoHA's approach includes establishing criteria against which to assess grant applications and appointing panels to assess the applications. Panel members are provided with a Guide for Assessors and assessment templates. The Guide includes the application forms and Program Guidelines. Services and the assessors expressed support for DoHA's process for assessing potential RTCM grants.
Negotiating funding agreements
DoHA has suitable procedures in place to negotiate and execute funding agreements with successful grant applicants. Generally, negotiations are documented and agreements are cleared by DoHA's LSB and CMAU. The negotiation process is reasonably timely and agreements are executed on DoHA's behalf by appropriate delegates. In interviews with the ANAO, services reported a good working relationship with DoHA.
Monitoring Grants
Project reporting
DoHA's process for assessing project reports is complex. Grant recipients are required to submit six-monthly project reports which are assessed by STOs using a standardised State/Territory Office—Project Report Assessment template. CO is then responsible for reviewing STO project report assessments. Once CO approves a project report, this triggers the next instalment of the service's grant payment.
The ANAO understands that it may have been necessary in the early stages of the program for CO to review all STO project report assessments. Nevertheless, as the program enters Round 3: 2007–08, DoHA could look for efficiencies in the process by adopting a risk-based approach to assessing and approving project reports.
Verifying data and paying grant instalments
DoHA has established an effective invoicing and payments system. Payments are generally made in a timely manner and, when necessary, DoHA's payments system includes procedures to reduce, withhold or recover payments. However, DoHA does not verify important data contained in project reports. The data in these reports is the basis upon which payments are made. Therefore, it is important that DoHA gains adequate assurance on the accuracy of the data received. Also, this will enhance DoHA's monitoring of services' progress and compliance with the conditions of funding agreements.
The RTCM budget for 2004–05 to 2006–07 is $28.5 million, while grant payments to services in the same period amounted to $9.12 million. The underspend is a result of the number of grants issued being less than those available, some applicants requesting less than the maximum available funding, and an unrealistic assumption that the grants would be executed on 1 July each year. In February 2007, DoHA received approval to reallocate funding within the RTCM program.
Department of Health and Ageings Response
The Department of Health and Ageing (DoHA) supports the recommendations of the performance audit into its administration of the Round the Clock Medicare: Investing in After Hours GP Services (RTCM) Program.
DoHA accepts that the performance management framework currently in place to monitor and assess the performance of the program against its stated objectives could be improved. It also acknowledges the need to evaluate the effectiveness of the program, and to adopt a more systematic, risk-based approach to the verification of data provided by funding recipients in project progress reports. To this end, the Department has commenced work to implement the audit's recommendations.
In addition to the recommendations, the ANAO has made a number of other suggestions to assist the Department improve its administration of the RTCM Program. These include, amongst others, ways for streamlining DoHA's processes for assessing project deliverables, and issues that could be addressed as part of the planned evaluation of the program. DoHA is grateful for the suggestions made by the ANAO and has already commenced action to implement some of these suggestions. However, whilst the Department will consider all suggestions for improvement to the administration of the program made by the ANAO, action to implement these suggestions will be dependent upon a thorough assessment by the Department of the relative costs and benefits, and resources required, to implement the ANAO's proposals.
Footnotes
1 Bettering the Evaluation and Care of Health Project, General Practice Activity in Australia 2005–06, General Practice Series No.19 [Internet]. Bettering the Evaluation and Care of Health Project, 17 January 2007, available from <http://www.aihw.gov.au/publications/gep/gpaa05-06> [accessed 30 August 2007] p.79.
2 Health and Ageing Portfolio, Portfolio Budget Statements 2005–06: Budget Related Paper No. 1.11, May 2005, p. 90.