Browse our range of reports and publications including performance and financial statement audit reports, assurance review reports, information reports and annual reports.
Auditor-General Report No. 32 of 2015–16
Administration of Rehabilitation Services under the Military Rehabilitation and Compensation Act 2004
Published
Thursday 5 May 2016

Portfolio
Defence
Entity
Department of Defence; Department of Veterans' Affairs
Contact
Please direct enquiries relating to reports through our contact page.
Activity
Service delivery
Sector
Defence
Veterans' Affairs
The audit objective was to assess the effectiveness of the Department of Veterans' Affairs and Department of Defence's administration of rehabilitation services under the Military Rehabilitation and Compensation Act 2004.
Summary and recommendations
Background
1. The Military Rehabilitation and Compensation Act 2004 (MRCA) was introduced to bring together rehabilitation and compensation provisions for all serving and former members of the Australian Defence Force (ADF) regardless of the type of service performed for injuries and illnesses from service rendered on or after 1 July 2004. Although predecessor schemes exist and remain in operation1, the MRCA is the most relevant rehabilitation and compensation legislation for current serving ADF members and cadets.
2. There are many parallels between the MRCA and civilian workers’ compensation schemes including a focus on rehabilitation and return to work outcomes where possible. Initial rehabilitation services are delivered to serving ADF members through the ADF Rehabilitation Program. However, many of the significant longer-term costs and the ongoing liabilities for the Commonwealth arising from illness and injury within the Department of Defence (Defence) are met by a separate entity, the Department of Veterans’ Affairs (Veterans’ Affairs). The MRCA is administered by Veterans’ Affairs primarily through the Military Rehabilitation and Compensation Commission (MRCC). Defence is represented on the MRCC by two senior ADF serving members.
The Department of Defence
3. ADF personnel frequently operate in high risk environments, whether during training or on deployment. The downstream impacts arising from preventable workplace injuries and illness are significant, affecting both deployment capability and healthcare costs in the ADF as well as MRCA liabilities administered by Veterans’ Affairs.
4. In recognition of the importance of preventing injury and illness, Defence introduced its Work, Health and Safety Strategy 2012–17 that aims to ensure that, ‘no person will suffer a serious preventable work related injury or illness’. Defence undertakes its role as a rehabilitation authority under the MRCA through the ADF Rehabilitation Program which is delivered as an extension of the healthcare provided to ADF members. Healthcare and rehabilitation are provided to ADF members regardless of whether the injury or illness is workplace-related. The ADF Rehabilitation Program received 5013 referrals in 2013–14.2 The Army accounted for 63 per cent of referrals, the Navy 21 per cent and the Air Force 16 per cent.
Transition Services
5. Transition services prepare ADF members (including injured and ill members) for civilian life. The respective responsibilities of Defence and Veterans’ Affairs are recognised in legislation under the MRCA. In 2007, Defence committed to provide the men and women of the ADF with ‘exemplary support services, throughout their career, (and) particularly at the time of separation’. In 2013–14, there were 950 medical separations from the approximately 5000 ADF personnel referred to rehabilitation—almost 20 per cent.
Rehabilitation in the Department of Veterans’ Affairs
6. In addition to compensation payments under MRCA and predecessor schemes, rehabilitation services are core business for Veterans’ Affairs, whose approach is aimed at transitioning clients to civilian work and maximising quality of life for veterans after an injury or illness related to ADF service. There were 20 164 MRCA clients with Veterans’ Affairs as at September 2015 which included 1805 open (actively managed) rehabilitation cases. The majority of MRCA clients are of working age–over 85 per cent were less than 50 years as at March 2015.
7. Clients receiving rehabilitation may also receive incapacity payments (income maintenance)3 from Veterans’ Affairs. Veterans’ Affairs reported MRCA rehabilitation-related expenditure, including medical and incapacity payments, of $149 million in 2015. Behind this, however, is a much larger liability. The Australian Government Actuary estimated that, as at June 2015, the MRCA liability (including accepted claims and future liabilities) was $4.56 billion, up from $3.84 billion as at 30 June 2014.
Audit objective and criteria
8. The objective of this audit was to assess the effectiveness of Defence and Veterans’ Affairs administration of rehabilitation services under the Military Rehabilitation and Compensation Act 2004.
9. To form a conclusion against this objective, the ANAO adopted the following high-level criteria:
- Defence and Veterans’ Affairs have established appropriate and effective governance and coordination arrangements to facilitate their administration of rehabilitation services under the MRCA; and
- Defence and Veterans’ Affairs administration of rehabilitation services has a strong client focus that is consistent with legislative and policy requirements and is achieving intended outcomes.
Conclusion
10. ADF members and veterans are provided access to a wide range of rehabilitation and support services nationally through the ADF Rehabilitation Program and rehabilitation services provided through Veterans’ Affairs.
11. In managing rehabilitation programs, neither Defence nor Veterans’ Affairs reliably measure, monitor or report on outcomes. Civilian rehabilitation schemes, for example, use critical measures of performance; namely the timeliness of rehabilitation following injury or illness, and the durability of return to work outcomes. Accrued liabilities under the MRCA are significant and growing. Robust performance information has not been sufficiently developed or used by Defence and Veterans’ Affairs to manage the MRCA scheme overall, from assessing the risks of injury and illness in Defence through to considering the impact of rehabilitation on the overall performance and financial sustainability of the scheme.
12. The return to work rate, a third key indicator of the effectiveness of rehabilitation services, is significantly lower than the national benchmark—54 per cent for Veterans’ Affairs and 55 per cent for the ADF, compared with the Australian average of 77 percent in 2013–14. The rate of medical separations from the ADF has increased from 12 to 19 per cent of people leaving the ADF between 2010 and 2015.4 There has been a significant decline in the rate of transition to civilian work for Veterans’ Affairs rehabilitation clients from 66 per cent to 48 per cent over the same period.
Supporting findings
Prevention and rehabilitation of injuries and illness in the Australian Defence Force
13. Performance data within Defence is not sufficiently reliable or consistent across years to determine whether preventable injuries and illnesses, which have a downstream impact on deployment capability and MRCA liabilities, have reduced since the introduction of its Work Health and Safety Strategy in 2012. Defence has acknowledged that not all serious incidents are reported as not all parts of Defence have access to the reporting system, such as Navy vessels at sea and Cadets. Further, the ANAO was informed during numerous audit interviews with a range of ADF staff of reluctance within some parts of the ADF to report incidents due to perceived potential negative career impacts.
14. The performance measurement framework for the ADF Rehabilitation Program is poorly developed and does not measure performance against all key indicators. Therefore the ADF is unable to measure the overall effectiveness of rehabilitation services. While the ANAO notes that differing methodologies for determining the rates of return to work may limit a strict comparison, the available information indicates that the return to work rate is relatively low in comparison with other benchmarks, such as the national average for return to work post-rehabilitation. Defence has not sufficiently prioritised the capture of reliable return to work data and does not measure whether the return to work rate is lasting (durable) following rehabilitation and does not capture the extent to which rehabilitation is timely (that is, occurs as soon as practicable after injury or illness). These elements are recognised in the wider workers compensation sector as key factors for successful rehabilitation.
15. Defence does not effectively manage the costs of ADF rehabilitation services as it does not record the full cost of the ADF Rehabilitation Program.
16. The total value of rehabilitation-related expenditure in Defence is unknown as rehabilitation services, which are delivered through the Joint Health Command, is reported as part of the total ADF health costs. Only the outsourced case assessment and management component is separately identifiable. Within this category, expenditure has doubled to $19.94 million in the three years to 2015, reflecting the higher demand for rehabilitation service provision. The capture of limited financial data for rehabilitation means that Defence is unable to analyse or report accurately on expenditure for individual rehabilitation cases or for the rehabilitation function overall.
Transition Services for Injured and Ill ADF Personnel
17. There are a wide range of single-service (that is, Army, Navy or Air Force) and Defence-wide transition services available to the increasing number of ADF personnel who are discharged for medical reasons. However, Defence and Veterans’ Affairs cannot yet demonstrate through comprehensive and reliable performance information whether the support provided is effective and efficient in assisting transition to civilian life or which services provide the best results for injured and ill ADF personnel discharged for medical reasons.
Rehabilitation Services in the Department of Veterans’ Affairs
18. Despite rehabilitation services being core business for Veterans’ Affairs, there is no comprehensive performance data available to indicate whether rehabilitation services are effectively meeting the needs of veterans. Available data shows a substantial decline in successful rehabilitation outcomes for veterans with a return to work goal over the five years to 2015, suggesting that rehabilitation services by Veterans’ Affairs may be becoming less effective. Veterans’ Affairs have reported that a recent rehabilitation pilot project in South East Queensland that focussed on timely engagement and closer cooperation between Defence and Veterans’ Affairs demonstrated some improvements in the transition experience for members medically separating from Defence. While not conclusively demonstrating better outcomes from early engagement, 58 per cent of project participants successfully found work during the pilot period.
19. Veterans’ Affairs does not have a basis to demonstrate that its rehabilitation services represent value for money. Veterans’ Affairs has not completed market testing or established service level agreements with rehabilitation service providers to monitor and manage performance, and there is no documented rationale for selecting one provider over another when clients are referred to rehabilitation providers.
20. Incapacity payments have not been well managed to date. In 2014, Veterans’ Affairs reported a 22 per cent critical error rate in payments, against a target of five per cent. At the time of the audit, Veterans’ Affairs advised the ANAO that it was in the process of addressing the high error rates and complaints by MRCA clients through system and process improvements, as well as considering policy adjustments.
21. MRCA–related rehabilitation expenditure by Veterans’ Affairs has more than doubled to $149 million over the four years to 2015 and incapacity payments to support ADF personnel and veterans represent a substantial portion of this—$94 million in expenditure in 2015.
22. Since inception, MRCA liabilities have grown substantially each year to $4.5 billion at 30 June 2015, of which $2.37 billion relates to incapacity payments. The growth reflects the demand-driven nature of the scheme, which is funded through an essentially unlimited special appropriation. Available performance information does not yet enable an understanding of the contribution that rehabilitation services make to the financial sustainability of the MRCA.
Recommendations
|
Recommendation No 1 Paragraph 2.9 |
To improve the management of injury risks and downstream rehabilitation costs and MRCA liabilities arising from ADF workplace incidents, the ANAO recommends that the Department of Defence implement agency-wide use of the incident, injury and illness reporting system (‘Sentinel’) by all ADF personnel. The Department of Defence’s response: Agreed. |
|
Recommendation No 2 Paragraph 2.29 |
To measure the effectiveness of rehabilitation service delivery and to promote improved rehabilitation outcomes, the ANAO recommends that the Department of Defence:
The Department of Defence’s response: Agreed with qualification. (The qualification relates to making the measures more relevant to military personnel rather than civilian workers.) |
|
Recommendation No 3 Paragraph 3.17 |
To improve the effectiveness and efficiency of transition services to support injured and ill ADF personnel to find suitable civilian work, the ANAO recommends that the Departments of Defence and Veterans’ Affairs collect and analyse data to identify which transition support services and coordination approaches are associated with the best and most durable rehabilitation outcomes leading to civilian employment. The Department of Defence’s response: Agreed. The Department of Veterans’ Affairs’ response: Agreed. |
|
Recommendation No 4 Paragraph 4.13 |
To enhance measurement and reporting and to improve over time the effectiveness of rehabilitation services, the ANAO recommends that the Department of Veterans’ Affairs introduce:
The Department of Veterans’ Affairs’ response: Agreed. |
|
Recommendation No 5 Paragraph 4.27 |
In order to improve the management of rehabilitation service delivery and the rationale for selecting external rehabilitation service providers, the ANAO recommends that the Department of Veterans’ Affairs:
The Department of Veterans’ Affairs’ response: Agreed. |
Summary of entity responses
Department of Defence
Defence thanks the ANAO for the audit and acknowledges the findings contained in the audit report on the Administration of Rehabilitation Services under the Military Rehabilitation and Compensation Act 2004. Defence agrees with the three recommendations pertinent to the Department.
Department of Veterans’ Affairs
The Department of Veterans’ Affairs was pleased with the outcomes of the audit and thanks the Australian National Audit Office for the opportunity to respond to the issues raised.
1. Background
Introduction
1.1 The Military Rehabilitation and Compensation Act 2004 (MRCA) is the most relevant rehabilitation and compensation legislation for current serving Australian Defence Force (ADF) members and cadets.5 Amendments to the MRCA in 2013 were designed to further enhance rehabilitation services and the management of transition to civilian life for ADF members who are discharged for medical reasons.6
1.2 The aim of rehabilitation through the MRCA is to:
maximise the potential to restore a person who has an impairment, or an incapacity for service or work, as a result of a service injury or disease to at least the same physical and psychological state, and at least the same social, vocational and educational status, as he or she had before the injury or disease.7
1.3 The MRCA includes a focus on rehabilitation and return to work outcomes where possible. Initial rehabilitation services are delivered to serving ADF members through the ADF Rehabilitation Program, with the ongoing liabilities for the Commonwealth arising from illness and injury within the Department of Defence (Defence) being met by the Department of Veterans’ Affairs (Veterans’ Affairs).
1.4 Entities are also required to meet the provisions of the Public Governance Performance and Accountability Act 2013. In particular, this Act requires entities to:
- establish an appropriate system of risk oversight and management;
- measure and assess the entity’s performance; and
- promote the proper use and management of public resources and financial sustainability of the entity.
Prevention and rehabilitation of injury and illness in the Australian Defence Force
1.5 Following the introduction of the Work Health and Safety Act 2011, Defence introduced its Work, Health and Safety Strategy 2012–17 that aims to ensure that, ‘no person will suffer a serious preventable work related injury or illness’. When injuries or illness do occur to serving members of the ADF, rehabilitation services play an important role in recovery and returning members to work and maintaining Defence capability.
1.6 Defence undertakes its role (with the Chief of the Defence Force) as a rehabilitation authority8 under the MRCA (and the earlier Safety, Rehabilitation and Compensation Act 1988) through the ADF Rehabilitation Program, which was introduced in 2006. Rehabilitation services are delivered by Defence’s Joint Health Command. Occupational rehabilitation services are delivered as an extension of the healthcare provided to ADF members, regardless of whether the cause of the injury or illness is work-related. Referral to the ADF Rehabilitation Program is provided to reduce the impact of injury or illness and to maximise military capability through a return to work if possible.
1.7 The ADF Rehabilitation Program received 5013 referrals in 2013–149, an average annual increase of 4.4 per cent since 2008–09. The Army accounted for 63 per cent of referrals, the Navy 21 per cent and the Air Force 16 per cent. The types of injuries are outlined in Table 1.1.
Table 1.1: Injury Groups for New Referrals to Rehabilitation 2013–14
|
Injury Group |
Number |
Percent of Total |
|
Physical such as musculoskeletal conditions |
3620 |
72.2 |
|
Mental Health conditions |
869 |
17.3 |
|
Medical such as obesity, cancer, or cardiac conditions |
499 |
10.0 |
|
Other including insufficient categorisation detail |
25 |
0.5 |
|
Total |
5013 |
100.0 |
Source: Department of Defence ADF Rehabilitation Program Annual Report 2013–14, p.4.
Transition services and interaction between Defence and Veterans’ Affairs
1.8 Transition services prepare injured and ill ADF members for civilian life. The respective responsibilities of Defence and Veterans’ Affairs are recognised in legislation under the MRCA. In 2007, Defence committed to provide the men and women of the ADF with ‘exemplary support services, throughout their career, (and) particularly at the time of separation’.10
1.9 There are a number of means by which Defence and Veterans’ Affairs coordinate on rehabilitation services and provide service delivery for injured and ill ADF members during their transition to civilian life. Defence is represented on the Military Rehabilitation and Compensation Commission by two senior ADF serving members. In addition, Defence and Veterans’ Affairs have a memorandum of understanding (the Memorandum), aimed at both departments delivering ‘the best possible outcomes to ADF members, past and present and their eligible families’. The Memorandum sets out the framework of roles and responsibilities for the joint management of the Support Continuum—the coordinated and integrated system of support for wounded, injured or ill ADF members that extends across both departments, covering seven key processes:
- prevention;
- health care and recovery;
- liability determination;
- member support;
- return to work;
- transition; and
- post-transition care and support.
1.10 There are two governance structures responsible for managing the Memorandum: the Defence/Veterans’ Affairs Executive Committee which sets the joint strategic direction and the Defence/Veterans’ Affairs Links Steering Committee11, which has the operational role of ‘initiation and oversight of joint programs, projects or initiatives aimed at improving the way eligible wounded, injured or ill ADF members, and their families, are supported and cared for’.
1.11 The key points of interaction between Defence and Veterans’ Affairs are outlined in Figure 1.1, noting that a claim can be lodged with Veterans’ Affairs at any stage of a member’s career.
Figure 1.1: Overview of key rehabilitation processes

Note 1: Both serving and former members are able to lodge a claim with Veterans’ Affairs.
Note 2: For current serving members, Defence normally provides health and rehabilitation services.
Note 3: Compensation payments and these other services are provided by Veterans’ Affairs to serving and former members.
Source: ANAO analysis based on data from Defence and Veterans’ Affairs.
Rehabilitation in the Department of Veterans’ Affairs
1.12 In addition to compensation payments under MRCA and predecessor schemes, rehabilitation services are a core function for Veterans’ Affairs, whose approach is aimed at transitioning clients to civilian work and maximising quality of life for veterans after an injury or illness related to ADF service. There were 20 164 MRCA clients with Veterans’ Affairs as at September 2015, which included 1805 open rehabilitation cases.12 The majority of MRCA clients are of working age—over 85 per cent were under 50 years as at March 2015.
1.13 Clients receiving rehabilitation may also receive incapacity (income maintenance)13 payments from Veterans’ Affairs. Veterans’ Affairs reported MRCA rehabilitation-related expenditure, including medical and incapacity payments, of $149 million in 2015. Behind this, however, is a much larger liability. The Australian Government Actuary estimated that, as at June 2015, the MRCA liability (including accepted claims and future liabilities) was $4.56 billion14, up from $3.84 billion as at 30 June 2014.
1.14 The top five currently accepted conditions for those veterans who received rehabilitation through Veterans’ Affairs from cases closed in 2014–15 are shown in Table 1.2.
Table 1.2: Top five accepted conditions for those veterans receiving rehabilitation from cases closed in 2014–15
|
Top five accepted conditions from closed cases 2014–15 |
Number of Veterans |
|
Lumbar Spondylosis and other back problems |
240 |
|
Major depression/depressive disorder |
215 |
|
Tinnitus (ringing or buzzing in the ears) |
180 |
|
Post-traumatic Stress Disorder |
161 |
|
Osteoarthritis of a joint/s |
116 |
Note 1: Any individual could have more than one condition at a particular point in time.
Source: Veterans’ Affairs’ data 2014–15.
Previous reviews audits
1.15 The care of current and former ADF personnel has been the subject of a number of Parliamentary and internal reviews, including:
- the Senate Committee on Foreign Affairs, Defence and Trade inquiry into the mental health of ADF serving personnel (March 2016);
- the June 2013 inquiry of the Joint Standing Committee on Foreign Affairs, Defence and Trade into the Care of ADF Personnel Wounded and Injured on Operations report;
- the February 2011 report of the Review of Military Compensation Arrangements, conducted by Veterans’ Affairs in response to ex-service organisations’ concerns about some aspects of the MRCA, including the transition from previous legislation, and the interactions between the different pieces of legislation15; and
- in 2010, Defence’s Joint Health Command commissioned a review of the ADF’s current practices in supporting injured and ill ADF personnel.16
1.16 Two recent Australian National Audit Office (ANAO) audits touched on aspects of the administration of the MRCA. These were Administration of Mental Health Initiatives to Support Younger Veterans, and Management of Complaints and Other Feedback by the Department of Veterans’ Affairs.17
Audit Approach
1.17 The objective of this audit was to assess the effectiveness of Defence and Veterans’ Affairs administration of rehabilitation services under the Military Rehabilitation and Compensation Act 2004.
1.18 To form a conclusion against this objective, the ANAO adopted the following high-level criteria:
- Defence and Veterans’ Affairs have established appropriate and effective governance and coordination arrangements to facilitate their administration of rehabilitation services under the MRCA; and
- Defence and Veterans’ Affairs administration of rehabilitation services has a strong client focus that is consistent with legislative and policy requirements and is achieving intended outcomes.
1.19 The audit scope focused on rehabilitation services administered by the two entities and the extent to which these have achieved their intended outcomes. The audit did not examine individual client cases in detail or consider the merits of liability and compensation decisions. That is, the audit examined Defence and Veterans’ Affairs governance management systems, processes and overall outcomes following referral to rehabilitation services.
1.20 The audit involved the assessment of practices and examination of documentation against legislative and policy requirements and better practice, interviews with key staff and stakeholders and extraction and analysis of data. The audit team travelled to major Army, Navy and Air Force bases, Defence and Veterans’ Affairs offices, service providers and ex-service organisations. Submissions were also invited from service providers, peak ex-service organisations, and the community through the ANAO’s citizen input portal.
1.21 The audit was conducted18 in accordance with ANAO Auditing Standards at an approximate cost to the ANAO of $542 857.
2. Prevention and rehabilitation of injuries and illness in the Australian Defence Force
Areas examined
This chapter examines the extent to which Defence has effectively managed the prevention of risks from injuries and illness within the Australian Defence Force (ADF) and the effectiveness of the rehabilitation program when injuries and illness occur.
Conclusion
Defence is a high risk environment for personnel engaged in war-like activities. Performance data within Defence is not sufficiently reliable or consistent across years to determine whether preventable injuries and illnesses, which have a downstream impact on deployment capability and Military Rehabilitation and Compensation Act 2004 (MRCA) liabilities, have reduced since the introduction of its Work Health and Safety Strategy in 2012.
Defence does not reliably measure, monitor or report on key performance outcomes using indicators. Civilian rehabilitation schemes, for example, use recognised critical measures of performance. Latest available data shows that the ADF return to work rate, a key indicator of the effectiveness of rehabilitation services, is at 55 per cent (2013–14). This is a relatively low success rate and does not compare well with other benchmarks, such as the Australian average of 77 percent in 2014.
Areas for improvement
The ANAO has made two recommendations aimed at improving the measures of injury prevention and the effectiveness of rehabilitation.
Introduction
2.1 The ADF has a requirement for a trained and fit workforce that has the capacity for deployment. Achieving this goal is not without risks. The training requirements for deployment are rigorous and demanding and almost 60 per cent of total reported incidents arise from training. The ADF deployments from 1999 to 2015 to East Timor, the Solomon Islands, Iraq and Afghanistan have also exposed ADF personnel to significant risks to their health and wellbeing as part of military operations. When prevention of injuries or illness cannot be achieved, ADF healthcare and rehabilitation services provide the basis for returning ADF personnel to work in the ADF or alternatively to be prepared for separation to civilian life. In examining rehabilitation, the ANAO focussed on:
- the prevention and management of risks of injuries and illness;
- the effectiveness of rehabilitation services; and
- managing costs of ADF rehabilitation services.
Is Defence effectively managing the risks of injuries and illness in the ADF?
Performance data within Defence is not sufficiently reliable or consistent across years to determine whether preventable injuries and illnesses, which have a downstream impact on deployment capability and MRCA liabilities, have reduced since the introduction of its Work Health and Safety Strategy in 2012. Defence has acknowledged that not all serious incidents are reported as not all parts of Defence have access to the reporting system, such as Navy vessels at sea and Cadets. Further, the ANAO was informed during numerous audit interviews with a range of ADF staff of reluctance within some parts of the ADF to report incidents due to perceived potential negative career impacts.
2.2 Downstream impacts arising from preventable workplace injuries and illness are significant, particularly in a high-risk environment like the ADF, and affect both deployment capability in the ADF and MRCA liabilities administered by Veterans’ Affairs. In 2011, new national workplace health and safety legislation (the Work Health and Safety Act 2011) was introduced and provided a national framework that required Defence to focus on maximising the prevention of injury and illness and minimising the impact of any injury that does occur.
2.3 Defence has introduced a Work, Health and Safety Strategy 2012–17 (the strategy) that aims to ensure that, ‘no person will suffer a serious, preventable work related injury or illnesses’.19 The implementation of the strategy involves the provision of information, policy, guidance, training and leadership and a strengthened focus on reporting incidents through the enterprise-wide Work Health and Safety Management System, Sentinel. The Sentinel system also aims to capture why the incident occurred and what reasonable steps can be taken to prevent a reoccurrence. The Defence Work, Health and Safety Committee (DWHSC)20 provides the oversight and governance to encourage a consistent approach to safety across all areas of Defence.
2.4 Defence reported to its DWHSC in August 2015 that there had been a steady decline in the number of dangerous incidents across ADF members and Defence APS (civilian) employees21 from 1720 in 2010–11 to 641 in 2014–15—a 62.7 per cent decline. The number of fatalities recorded varied between eight and thirteen per annum from 2010–11 to 2014–15.
2.5 These results appear positive. However, there have been significant changes in the requirements for reporting since 2013, including the type of incidents that need to be reported and how incidents are reported. Factors such as changes in legal definitions of notifiable events (including the new ‘near miss’ category22 introduced in 2013–14 to improve the management of high risk incidents) have made it difficult to compare meaningful changes in performance over time.
2.6 Defence has acknowledged access to the Sentinel system is constrained for some groups. For example, Navy and many other parts of the ADF and Cadets do not have ready access to the Defence Restricted Network–making it harder to log incidents in the Sentinel system. Sentinel is not yet available in disconnected environments, such as on Naval vessels on deployment. There are also various systems that have been in place for some time within particular services that are not integrated with Sentinel.
2.7 Further, the ANAO was informed during numerous audit interviews with a range of ADF staff that there is reluctance within some parts of the ADF to report injuries or illness due to potential negative career impacts. Under-reporting of incidents and injuries impacts on the ability of Defence to monitor trends over time, properly manage risks and demonstrate compliance with its legislative requirements.
2.8 As a result, 2014–15 data is not comparable with previous years, and any trend analysis is potentially misleading. Defence has recognised its data limitations and has advised the ANAO that it is investigating rates of injuries against national standards for future reporting purposes. Strengthened efforts are required to address the underreporting of incidents, injuries and illness.
Recommendation No.1
2.9 To improve the management of injury risks and downstream rehabilitation costs and MRCA liabilities arising from ADF workplace incidents, the ANAO recommends that the Department of Defence implement agency-wide use of the incident, injury and illness reporting system (‘Sentinel’) by all ADF personnel.
Department of Defence response: Agreed.
2.10 Defence has agreed with this recommendation and has provided the follow comment:
2.11 ‘Defence is already implementing this recommendation. In accordance with Joint Directive 27/2014, all members of the ADF are required to use Sentinel to report work related injury and illness. Since its introduction Sentinel has seen ongoing improvement to improve the ease with which Defence personnel can report individuals who suffer work related injury or illness. Defence has arrangements in place for events/incidents to be recorded in Sentinel where access is not yet available, and is working with the software owner to address this gap. Defence acknowledges that aligning a new standardised reporting arrangement with diverse business processes requires ongoing attention. The Defence Work Health and Safety Committee considers Sentinel implementation at their quarterly meetings. A new version of Sentinel was released on 29 Feb 2016. A suite of new Sentinel training products for all Defence personnel will be released in May 2016. These are all activities designed to support the Agency wide use of Sentinel. This in turn is expected to contribute to reducing risks and related MRCA liabilities through more accurate data and analysis of incidents/injuries and illnesses.’
How effective are ADF rehabilitation services?
The performance measurement framework for the ADF Rehabilitation Program is poorly developed and does not measure performance against all key indicators. Therefore the ADF is unable to measure the overall effectiveness of rehabilitation services. While the ANAO notes that differing methodologies for determining the rates of return to work may limit a strict comparison, the available information indicates that the return to work rate is relatively low in comparison with other benchmarks, such as the national average for return to work post-rehabilitation. Defence has not sufficiently prioritised the capture of reliable return to work data and does not measure whether the return to work rate is lasting (durable) following rehabilitation and does not capture the extent to which rehabilitation is timely (that is, occurs as soon as practicable after injury or illness). These elements are recognised in the wider workers’ compensation sector as key factors for successful rehabilitation.
2.12 The purpose of rehabilitation activity in Defence is to return people to work if possible, or to support them to transition out of the ADF to civilian life. High quality performance information is necessary to identify whether Defence’s rehabilitation services are effective and facilitates sound decision-making to manage risks and service delivery.
The ADF Rehabilitation Program
2.13 Upon referral23 to the ADF Rehabilitation Program one of three goals is assigned to injured or ill members:
- Goal 1—fit for duty in the pre-injury/illness work environment;
- Goal 2—fit for alternative duty in the ADF; or
- Goal 3—transition out of the ADF.
2.14 Since 2012, delivery has involved both internal and external service providers. As at 30 June 2015, the ADF Rehabilitation Program had 53 full-time equivalent internal Defence staff allocated to either rehabilitation case coordination and/or case management and located in major military bases around Australia. External rehabilitation services are available through Defence’s contract with Medibank Health Solutions. While the contract is non-exclusive (Defence can access any rehabilitation service provider in the community), Medibank Health Solutions has made arrangements with Advanced Personnel Management and Konekt to deliver occupational rehabilitation services to the ADF.24
2.15 New referrals for rehabilitation increased from 4117 in 2008–09 to 5013 in 2013–1425 —a 21.8 per cent increase over five years. In June 2014 there were 3967 open (active) cases compared with 2285 open cases in June 2010. Figure 2.1 illustrates Defence’s referrals, closed cases (no longer active) and open cases for the ADF Rehabilitation Program.
Figure 2.1: Referrals, closed cases and open cases for the ADF Rehabilitation Program 2008–09 to 2013–14

Source: ANAO analysis based on Defence data (2008–09 open case data not available).
2.16 Defence advised the ANAO that the increased number of referrals to rehabilitation has been driven by the level of overseas deployments in war-like conditions and the training/readiness cycle for ADF personnel.
Performance measurement for the ADF Rehabilitation Program
2.17 There are three indicators recognised in the workers’ compensation sector, including by Comcare26 and private rehabilitation providers, as important for measuring successful rehabilitation. These are the time from injury or illness to rehabilitation (timeliness of referral)27, the return to work rate and the durability of return to work outcomes (longevity). Measuring and tracking these indicators requires reliable systems and data.
ADF Rehabilitation Systems
2.18 Defence’s capture of reliable data has been hampered by poor contract specification and system capability. The contract for outsourced rehabilitation services does not have explicit deliverables or rehabilitation performance reporting requirements for outsourced rehabilitation service providers.
2.19 Since February 2015 when the ADF rehabilitation case management database28 was closed, there has been no electronic case management capability to enable efficient case management and from which related performance information can be extracted. Although the ADF Rehabilitation Program is delivered as part of health service delivery, Defence’s eHealth system does not have a rehabilitation management function, reinforcing findings of a previous audit in which the ANAO found that Defence’s eHealth system was beset by poor planning, governance and cost blow-outs and at December 2014 cost $133.3 million.29
2.20 Defence has advised the ANAO that an automated reporting capability is being developed for rehabilitation services with a potential rollout anticipated in the longer term. In the meantime, as part of the Rehabilitation Healthcare Improvement Project a case tracking spreadsheet has been developed and rolled out from January 2016. This has been designed to achieve better data capture in the interim.
ADF Rehabilitation Data
2.21 Following changes to incident reporting and rehabilitation case management systems, Defence has not captured data on the time between injury or illness and referral to rehabilitation since the second half of 2011–12. Data from 13 297 cases before this time shows that 17 per cent took longer than 12 months from injury to referral. A report by an industry provider in 2013 found that those referred within the first two weeks after injury achieved a 97 per cent return to work rate compared with 83 per cent after 12 months.30
2.22 Defence provided data from 2008–09 to 2013–14. At the time of the audit, Defence was not able to provide the ANAO with complete or reliable data for 2014–15 on rehabilitation case numbers and return to work outcomes. Available data is presented in Figure 2.2, which illustrates the changes in the ADF return to work rate from 2008–09 to 2013–14 compared with an Australian average and a broadly comparable high risk occupation—NSW Firefighters.
Figure 2.2: Return to Work Data for the ADF compared with the Australian Average (Currently in Work) 2008–09 to 2013–14
 2008–09 to 2013–14")
Source: Department of Defence Rehabilitation Program data. The Social Research Centre (2014): Return to Work Survey: 2013/14 Headline Measures Report (Australia and New Zealand), p.4, and ANAO analysis of data from - Audit Office of NSW (2014): Fitness of Firefighters, pp 25-26.
2.23 ADF Rehabilitation Program return to work outcomes (Goal 1 and 2) are low in comparison with the national average and with NSW firefighters, another high risk industry, noting that the differing methodologies for determining the three categories limit a strict comparison.31 A low return to work rate has a cost impact from recruiting and training replacement ADF personnel. The ANAO has estimated32 that the cost of replacing medically-separated ADF personnel in 2013–14 was at least $60.7 million.
2.24 Defence does not have a measure of the durability of rehabilitation services or whether services result in lasting outcomes. Defence has advised the ANAO that they propose to implement a ‘return to duty’ rate to replace durability of return to work as a measure of sustainable rehabilitation outcomes in Defence. This rate would measure how many ADF members who received rehabilitation through the ADFRP and achieved a return to work outcome had returned to a deployable Medical Employment Classification at a defined period after the closure of their rehabilitation program. A proposal to implement this measure has been put to the Defence Work Health Safety Committee. This measure reflects that ADF members must achieve a higher level of function than a civilian employee in order to fully return to work.
Information for decision-making and performance management
2.25 The data currently collected and utilised by Defence is not comprehensive and provides only an incomplete basis for analysing rehabilitation program performance. In particular, the lack of continuity of data collection and reporting is a significant weakness in Defence’s performance measurement for the ADF Rehabilitation Program.
2.26 Defence’s Joint Health Command has been severely limited in its ability to report aggregated data on rehabilitation performance. The aggregation of data to identify opportunities at a national level for delivery efficiencies or to identify early illness and injury trends has been poorly developed, which has impacted the capacity to report to the Defence Executive or external bodies such as the Military Rehabilitation and Compensation Commission. Defence’s planned automated reporting capability scheduled for rollout in the latter half of 2016 seeks to address this limitation.
2.27 A 10-year study to examine ‘the effectiveness of rehabilitation arrangements under the MRCA over the long term’ has been recently commissioned by Defence and Veterans’ Affairs.33 The study’s objectives include, to:
- evaluate the long-term effectiveness of rehabilitation programs and services for serving and ex-serving ADF members taking into account all aspects of rehabilitation and impact on families;
- document trends in client outcomes over time which will include the types and severity of the injury;
- determine what factors are associated with better or worse rehabilitation outcomes in serving and ex-serving ADF members; and
- identify critical handover points between agencies during the rehabilitation process and opportunities to improve communication at these points.
2.28 Preliminary results will not be available until at least 2018. However, the ANAO considers that it will be important to progressively incorporate the study findings into improved performance management of the ADF Rehabilitation Program. The data gaps identified by the ANAO will have to be addressed by Defence for management information purposes and as inputs to the long-term study. The study alone will not address the ongoing management information gaps in Defence.
Recommendation No.2
2.29 To measure the effectiveness of rehabilitation service delivery and to promote improved rehabilitation outcomes, the ANAO recommends that the Department of Defence:
- improve monitoring and reporting of key rehabilitation performance indicators including timeliness between injury or illness and referral to rehabilitation, durability of return to work outcomes and the cost of rehabilitation services overall and on a case basis; and
- include performance trend data and analysis in internal management reporting and the Annual Report of the ADF Rehabilitation Program along with what actions have been taken to inform performance over time.
Department of Defence response: Agreed.
2.30 Defence has agreed with this recommendation and has provided the following qualification: ‘The use of measures used by civilian workers compensation jurisdictions are not applicable to the ADF and its health care and rehabilitation system. To meet the intent of the ANAO Report we have proposed measures more relevant to military personnel.’
Does Defence effectively manage the costs of the ADF rehabilitation services?
Defence does not effectively manage the costs of ADF rehabilitation services as it does not record the full cost of the ADF Rehabilitation Program.
The total value of rehabilitation-related expenditure in Defence is unknown as rehabilitation services, which are delivered through the Joint Health Command, is reported as part of the total ADF health costs. Only the outsourced case assessment and management component is separately identifiable. Within this category, expenditure has doubled to $19.94 million in the three years to 2015, reflecting the higher demand for rehabilitation service provision. The capture of limited financial data for rehabilitation means that Defence is unable to analyse or report accurately on expenditure for individual rehabilitation cases or for the rehabilitation function overall.
2.31 A contract between Defence and Medibank Health Solutions was introduced in 2012 and is valued at $1.3 billion over four years to deliver medical services, including rehabilitation. Direct expenditure on rehabilitation assessment and case management under the outsourced contract is a small part of the outsourced health services contract, representing $9.47 million in 2012−13 and increasing to $19.94 million in 2014–15 in response to increasing demand for services.
2.32 Defence does not separately capture information on total rehabilitation expenditure within its health budget. Individual rehabilitation cases can involve a package of health and other care services such as psychiatric services or other medical assistance depending on the needs of each person. Such costs are generally not explicitly classified as rehabilitation services.
2.33 The limited capture of financial data at a case level means that Defence is unable to analyse or report accurately on expenditure for individual rehabilitation cases or for the rehabilitation function overall. The absence of full cost information makes it more difficult for Defence to manage resources and assess the most cost effective means of delivering rehabilitation services.
2.34 In October 2015, Defence Joint Health Command was developing a revised service delivery model following on from a Rehabilitation and Healthcare Improvement Project. The purpose of the revised delivery model is to enhance the capacity of Defence to better meet the demand for rehabilitation services. Implementation is at an early stage and the project is not anticipated to be rolled out until later in 2016. The planned approach is based on new processes and governance arrangements. The ANAO considers that the cost effectiveness of the current or proposed approach cannot be determined unless Defence has a better understanding of the total costs of delivering the ADF rehabilitation program.
3. Transition services for injured and ill ADF personnel
Areas examined
This chapter examines the extent to which Defence and Veterans’ Affairs have provided support to the Australian Defence Force (ADF) personnel being medically discharged and how effective it has been in assisting their transition to civilian life.
Conclusion
The rate of medical separations from the ADF has increased from 12 to 19 per cent of people leaving the ADF between 2010 and 2015. Defence has advised the ANAO that much of the increase in discharge for medical reasons has been due to the tempo of deployment and associated intensive training over the past decade.
Previous reviews of rehabilitation and compensation for ADF members have highlighted issues with the consistency, coordination and duplication of transition services for those leaving the ADF. Governance arrangements have been strengthened and new initiatives introduced. Despite these measures, the transition experience for injured and ill ADF personnel remains lengthy, complex and inconsistent. The ANAO found that Defence and Veterans’ Affairs have not adequately assessed the effectiveness of the suite of transition services offered by both entities.
Areas for Improvement
The ANAO has made one recommendation designed to improve the coordination of transition services.
Introduction
3.1 The transition process is designed to aid and support all ADF members who are separating from the ADF to civilian life. Transition services are required under the Military Rehabilitation and Compensation Act 2004 (MRCA) for members discharged on medical grounds, some of whom will not have received rehabilitation services. The ADF has a duty of care to its personnel before separation, while post-separation matters are administered by Veterans’ Affairs for accepted conditions. Effective and efficient coordination between the two entities will facilitate a smooth transition.
Is the support provided to medically discharged ADF personnel effective and efficient in assisting their transition to civilian life?
There are a wide range of single-service (that is, Army, Navy or Air Force) and Defence-wide transition services available to the increasing number of ADF personnel who are discharged for medical reasons. However, Defence and Veterans’ Affairs cannot yet demonstrate through comprehensive and reliable performance information whether the support provided is effective and efficient in assisting transition to civilian life or which services provide the best results for injured and ill ADF personnel discharged for medical reasons.
Discharge from the ADF on medical grounds
3.2 The number of ADF members that are discharged on medical grounds has been increasing, as illustrated in Figure 3.1.
Figure 3.1: Medical discharge from the ADF as a proportion of total ADF separations, 2008–09 to 2014–15
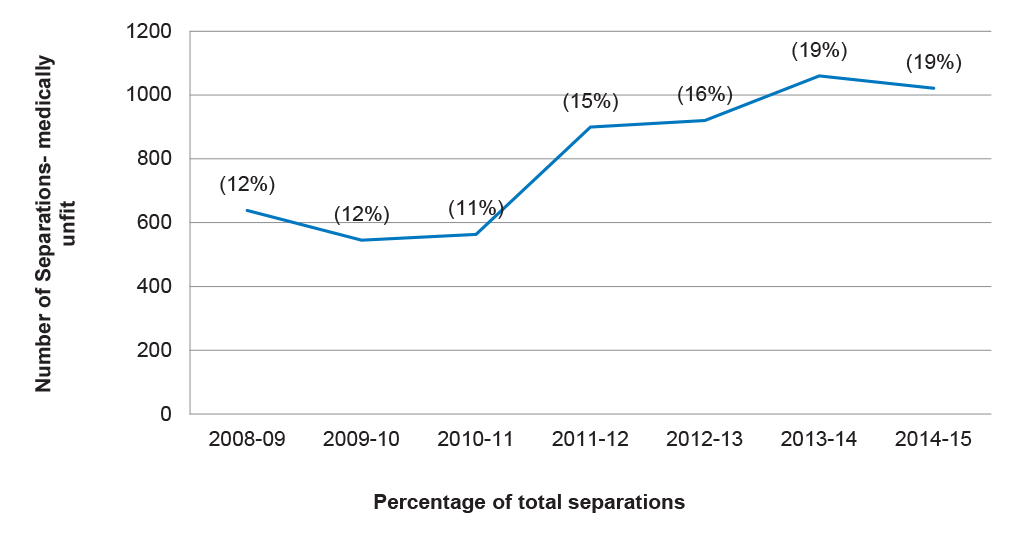
Source: ANAO analysis of Defence data.
The process of transition from the ADF
3.3 The MRCA requires the ADF to appoint a transition case manager for personnel discharged on medical grounds.34 When an ADF member is identified for medical discharge, they are subject to the Medical Employment Classification (MEC) process which is intended to facilitate the consistent application of medical advice regarding the employability and deployability of all ADF members. Classifications are regularly reviewed to ensure they are appropriate for the person’s employment circumstances.
3.4 Transition can be a long and complex process depending upon the circumstances of each ADF member. In the context of transition from the ADF, the trigger for commencing a transition pathway for a member is that they have been considered non-deployable for a period of greater than 12 months, or it is considered likely that their condition will mean they will not reach a deployable status within 12 months of the onset.
3.5 Figure 3.2 illustrates the process for a member being considered by the Medical Employment Classification Review Board (MECRB) following a member reaching a trigger point for the central MEC Board Review process.35
Figure 3.2: Timing of transition for injured or ill personnel who meet the trigger for a MEC Review Board review.

Source: ANAO analysis based on Defence documents and interviews with ADF personnel.
3.6 Figure 3.2 highlights that it can take up to 14 months without appeals or being held-in-abeyance36 for a member to transition from the ADF in addition to the time already in rehabilitation. The process is protracted and there is particular uncertainty for ADF members during the period of up to five months when their classification is being considered by the MEC Advisory Review Service (up to 3–4 months) and the MEC Review Board (some 2–4 weeks). Depending on the nature and/or severity of the transitioning member’s health condition, the process can take some years and involve retraining, or other forms of education and reskilling.
Support services available for injured and ill ADF members
3.7 For injured or ill members of the ADF in transition, there are a wide range of single-service options, as well as Defence-wide or Veterans’ Affairs services available.
3.8 Figure 3.3 provides a simplified diagram of support services for members in transition at the time of audit.
3.9 Figure 3.3 highlights the investment by both Defence and Veterans’ Affairs in providing services for injured and ill ADF members as well as the potential complexity for ADF members navigating the transition process. Some transition services are offered through the normal command and management structure on a single-service basis and others as part of Defence-wide support coordination. Services include Health and Wellbeing Officers located in Army Brigade Headquarters to provide advice and support to commanders, Soldier Recovery Centres (Army) and Personnel Support Units (Navy) to provide specific centres and programs that assist injured and ill ADF members.37 A range of transition services are also available to all transitioning ADF personnel, such as the Career Transition Assistance Scheme which provides vocational assessments, training and other assistance. For severely injured or ill ADF members, the Simpson Assistance Program is an initiative designed to reduce the impact of injury and illness by developing a tailored, integrated and multidisciplinary approach, to accelerated rehabilitation for seriously wounded, injured or ill members. This included a comprehensive approach to tailored recovery programs to support the individual needs of wounded ADF personnel, and their families and to assist and encourage ADF personnel, (with the support of their families) to return to the ADF workplace in either similar or new capacities.
3.10 The support pathways engaged will vary depending on circumstances, including whether the members’ originating units are on deployment or where the injury or illness is such that the ADF member and their families require additional resources.38 For members assessed as complex cases (those with more serious or multiple injuries or illnesses), Defence may appoint a Member Support Coordinator to assist the member through the process.
Figure 3.3: Support and information flow for ADF members in rehabilitation and transition on medical grounds

Source: ANAO analysis based on Defence and Veterans’ Affairs information.
3.11 From July 2013 to June 2015, the number of cases with a Member Support Coordinator varied between 466 and 700. There was no overall trend evident from the statistics over this time period. As at June 2015, there were 498 cases involving a Member Support Coordinator. While Member Support Coordinators are expected to improve the transition process for injured or ill ADF members, there is no evidence to indicate whether Members Support Coordinators are used in all necessary cases, or how effective or efficient they have been in supporting transitioning ADF members.
3.12 A new initiative adding to the range of services available is the Transition for Employment—a pilot program running from October 2015 to May 2016 aimed at Army personnel being medically separated. Its focus is on getting 150 members into civilian employment on their separation. The Army aims to evaluate the pilot with the view to a wider application of the program. Defence has advised that the Army is working in conjunction with the Defence Community Organisation and the participants in the pilot. One of the expected benefits of the pilot is that the preliminary work may result in a better targeted use of the Career Transition Assistance Scheme by members involved.
3.13 The range of services gives rise to a potential for overlap and inconsistency during the lengthy transition process for ill and injured ADF members.
Oversight and management of improvements in the coordination and delivery of transition services
3.14 The governance structures responsible for managing the Memorandum of Understanding between Defence and Veterans’ Affairs are designed to provide oversight and coordination for all relevant aspects of support for ill and injured ADF personnel including during transition. In particular as noted in Chapter 1, the Executive Committee is responsible, amongst other things, for ‘ensuring that the delivery of the care and support to eligible persons remains effective and coordinated, is delivered in the most appropriate and respectful manner’. In addition, the Links Steering Committee, responsible to the Executive Committee, receives a range of performance reports on all aspects of rehabilitation from injury prevention to care and support following transition. Initiatives such as the ‘single access mechanism’ have been implemented to assist in streamlining the flow of information from Defence to Veterans’ Affairs, and agreement has been reached to adopt a common identifier to allow the service delivery and outcomes of individuals to be tracked through both departments.
3.15 Despite the wide range of services being offered to transitioning members and the governance framework in place to ensure delivery of effective care and support. There are also no measures to provide information on how effective or efficient these initiatives have been and whether they could be streamlined or better coordinated for the future to avoid gaps or overlap in the services. There is no statistically valid information from injured or ill ADF personnel themselves on the effectiveness and value of transition services.39
3.16 A voluntary survey was conducted by Defence that provides an indication of the views of a small number (77 or 14.5 per cent) of medically separated ADF members in 2014—three to six months after their separation from the Defence force. Thirty-nine per cent of respondents considered that they were prepared for civilian life at separation. Of those receiving ADF Rehabilitation Program services in the lead up to separation, 36 per cent of respondents (45) considered that they were prepared for civilian life at separation. These results cannot be interpreted as generally reflecting the views of medically discharging ADF personnel. Nevertheless, they provide some indicative evidence that transition services could be improved. Collecting and analysing relevant data to identify transition support services that are associated with best rehabilitation outcomes in the context of the long-term study into the effectiveness of rehabilitation services would assist in shaping the future direction of transition services.
Recommendation No.3
3.17 To improve the effectiveness and efficiency of transition services to support injured and ill ADF personnel to find suitable civilian work, the ANAO recommends that the Departments of Defence and Veterans’ Affairs collect and analyse data to identify which transition support services and coordination approaches are associated with the best and most durable rehabilitation outcomes leading to civilian employment.
Entity responses: Agreed.
3.18 Defence and Veterans’ Affairs have agreed with this recommendation. Veterans’ Affairs has commented as follows:
3.19 ‘The Department of Defence has primary responsibility for members transitioning from the ADF. DVA actively supports Defence through a range of programmes which aim to connect with transitioning members as early as possible in the process.
3.20 The Departments of Defence and Veterans’ Affairs work together to facilitate a smooth transition for ADF members. Since 2010, Defence and DVA have been working together to implement the Support for Wounded Injured or Ill programme (SWIIP) to develop a whole of life framework (support continuum) for the care of wounded, injured or ill current and former serving ADF members. The responsibilities of each Department with respect to SWIIP are outlined in the Defence/DVA Memorandum of Understanding for the Cooperative Delivery of Care and Support for Eligible Persons (MoU).
3.21 Building on a pilot project of the Veterans’ Employment Assistance Initiative (VEAI) conducted in South East Queensland in 2014–15, DVA has commenced a timely engagement program with the Australian Defence Force (ADF) Rehabilitation Program to engage with individuals separating from the ADF on medical grounds at the earliest possible time prior to their separation. It provides an opportunity for a more effective handover of rehabilitation arrangements to DVA and to identify other areas of support required.
3.22 Phase 2 of the VEAI, which is currently being trialled in South Australia, enhances vocational rehabilitation within the context of DVA’s broader rehabilitation programs. Opportunities to better support clients, employers and rehabilitation providers will also be identified to assist clients in getting job ready and finding meaningful and sustainable employment and to improve the range and extent of employment opportunities for clients. Following completion of the trial, an evaluation will be undertaken and options will be developed for a national roll out of these arrangements.
3.23 DVA is starting to build a more complete picture of the effects of transition on ADF personnel. Through its research programs, DVA commenced collecting some data that may aid in identifying the best and most durable rehabilitation outcomes for ADF members, these include:
- MRCA Rehabilitation Long-Term Study–this will study the effectiveness of rehabilitation under the Military Rehabilitation and Compensation Act 2004 (MRCA).a joint research project, the broad aim is to evaluate the effectiveness of arrangements under the MRCA within the Australian Defence Force (ADF) and DVA over the long-term. This study commenced in February 2016.
- Transition Wellbeing Research Programme–will examine the impact of contemporary military service on the mental, physical, and social health of serving and ex-serving personnel and their families and builds on previous Defence research such as the Military Health Outcomes Program conducted in 2010. This programme commenced in June 2015.’
4. Rehabilitation services in the Department of Veterans’ Affairs
Areas examined
This chapter examines the extent to which Veterans’ Affairs delivery of rehabilitation services is effective and achieves value for money.
Conclusion
There is no comprehensive performance data available in Veterans’ Affairs to indicate whether rehabilitation services are effectively meeting the needs of veterans. Where available, data demonstrates a decline in successful outcomes for veterans with a return-to-work goal, suggesting that rehabilitation services by Veterans’ Affairs are becoming less effective. A recent pilot project in South East Queensland has demonstrated that improved return to work rates can be achieved.
There are no service-level agreements with rehabilitation providers that reflect the focus of the current Veterans’ Affairs delivery model. There is no documentation to support why particular providers have been selected for rehabilitation services and delivery providers are not provided with structured feedback on performance. The costs of providing rehabilitation services continue to rise along with the accrued liabilities for the Commonwealth.
Areas for improvement
The ANAO has made two recommendations designed to improve the measurement of performance from the services being delivered to veterans and enhance the disclosure of value for money.
Introduction
4.1 The principal aim for Military Rehabilitation and Compensation Act 2004 (MRCA) rehabilitation services delivered by Veterans’ Affairs is to enable clients to find suitable civilian work and where that is not possible due to limitations from the injuries or illness to enable them to have a quality of life.
4.2 Veterans’ Affairs case management of rehabilitation delivery is underpinned by three key principles:
- an emphasis on whole-of-person needs and psychosocial rehabilitation40;
- an integrated multidisciplinary approach41; and
- early intervention and continuity of care.
4.3 Rehabilitation coordinators within Veterans’ Affairs refer clients with accepted needs (related to military service) to private rehabilitation providers for assessment and service provision through an agreed rehabilitation plan. The rehabilitation plan provides the key control point for setting goals and rehabilitation priorities and for financial approval and case management. Rehabilitation plans can have a return to work or a quality of life focus or both depending on the age, circumstances and health status of the client.
How effective are rehabilitation services in meeting the needs of veterans?
Despite rehabilitation services being core business for Veterans’ Affairs, there is no comprehensive performance data available to indicate whether rehabilitation services are effectively meeting the needs of veterans. Available data shows a substantial decline in successful rehabilitation outcomes for veterans with a return to work goal over the five years to 2015, suggesting that rehabilitation services by Veterans’ Affairs may be becoming less effective. Veterans’ Affairs have reported that a recent rehabilitation pilot project in South East Queensland that focussed on timely engagement and closer cooperation between Defence and Veterans’ Affairs demonstrated some improvements in the transition experience for members medically separating from Defence. While not conclusively demonstrating better outcomes from early engagement, 58 per cent of project participants successfully found work during the pilot period.
Veterans’ Affairs rehabilitation performance information
4.4 At the time of the audit, Veterans’ Affairs did not measure or report comprehensively on the effectiveness of rehabilitation services. The department’s annual report largely reports on inputs and activity and does not provide a comprehensive summary of the outcomes from rehabilitation services.
4.5 Client record data was obtained and analysed by the ANAO to assess rehabilitation performance against the key measures of timeliness of referral and return to work and quality of life42 outcomes. Veterans’ Affairs does not routinely monitor and report this data or durability of rehabilitation outcomes for internal decision-making for service delivery and MRCA scheme management purposes.
Timeliness of referral
4.6 The timeliness of rehabilitation referrals is important as early intervention improves the effectiveness of vocational rehabilitation. The younger cohorts of MRCA clients can be expected to have a stronger interest in return to work compared with those covered by earlier legislation.
4.7 ANAO analysis identified that the time taken from injury or illness to rehabilitation referral in Veterans’ Affairs for the 934 cases closed in 2014–15 was more than two years in 43 per cent of cases, with a median time of 1.7 years.43 What is not clear from the data is whether rehabilitation was required earlier and the extent to which this was provided by the ADF while the member was still serving. This highlights the need to better understand the relative effectiveness of transition services (discussed in Chapter 3) for improved management of cases between Veterans’ Affairs and Defence.
Return to work and quality of life outcomes
4.8 Figure 4.1 illustrates closed rehabilitation plans identified by rehabilitation providers as having successful outcomes for quality of life and return to work cases closed in 2014–15. The outcomes are not mutually exclusive and clients can have both outcomes in their plans.
4.9 Of the 1786 plans with a return to work objective, the trend line was consistently in decline from 66 per cent in 2010–11 to 48 per cent in 2014–15. This compared with the 2014 national return to work average of 77 per cent following rehabilitation.44
Figure 4.1: Closed rehabilitation cases with successful outcomes 2010–2011 to 2014–15

Source: ANAO analysis based on Department of Veterans’ Affairs data.
4.10 From the 1316 quality of life plans examined from 2010–11 to 2014–15, success varied from 78 per cent to 82 per cent with no discernible trend. While the results are broadly positive, there is little documentation supporting what constitutes a quality of life outcome. Assessments are made by case managers and this could be better explained in the future to enable Veterans’ Affairs to compare results across providers and cases and assess implications for improved service delivery.
Veterans’ Affairs initiatives to improve rehabilitation services
4.11 Veterans’ Affairs and Defence have conducted a pilot project in South East Queensland to explore improved outcomes (Veterans’ Employment Assistance Initiative 2014–15). The pilot project tested a new arrangement to engage with members who were about to separate from the ADF with a service-related condition. Veterans’ Affairs have reported that a recent rehabilitation pilot project in South East Queensland that focussed on timely engagement and closer cooperation between Defence and Veterans’ Affairs demonstrated some improvements in the transition experience for members medically separating from Defence. While not conclusively demonstrating better outcomes from early engagement, 58 per cent of project participants successfully found work during the pilot period. Further, Veterans’ Affairs has advised the ANAO that it is also developing an Early Engagement Model which aims to identify, engage and support members from the point of joining the ADF onwards. The model aims to allow Veterans’ Affairs to influence the time taken by members to make a claim through early engagement and to reduce the time taken to process claims by having information on hand prior to a claim.
4.12 More broadly, Veterans’ Affairs has further advised the ANAO that it is introducing Goal Attainment Scaling as a standardised scoring system to assess and report on outcomes from rehabilitation services. Some of the expected benefits of Goal Attainment Scaling45 identified by the department include identifying the effectiveness of different types of rehabilitation and identifying areas for improvement. The approach is still in the early stages of implementation. The joint study with Defence of the effectiveness of rehabilitation arrangements under the MRCA over the long term may be able to assist in providing a more consistent, national focus for measuring outcomes.
Recommendation No.4
4.13 To enhance measurement and reporting and to improve over time the effectiveness of rehabilitation services, the ANAO recommends that the Department of Veterans’ Affairs introduce:
- relevant outcome measures and targets (including early intervention, return to work, quality of life and durability) as key performance indicators for rehabilitation services; and
- report against these measures to the Executive of Veterans’ Affairs and, where appropriate, include the information in the department’s annual report.
The Department of Veterans’ Affairs response: Agreed.
4.14 The Department of Veterans’ Affairs has agreed to this recommendation and provided the following comment:
4.15 ‘To assist in measuring key outcomes DVA is using the Goal Attainment Scaling (GAS) method to assess both individual activities and overall program goals. Analysis of these findings will allow DVA to gauge the viability and longevity of rehabilitation activities. A Program Performance Indicator for inclusion in the 2016–17 Program Budget Statement and Annual Report specifically relates to this recommendation. DVA will continue to investigate opportunities to measure outcomes including use of the MRCA Review Long-Term Study into Rehabilitation Phase One Study Design to identify metrics around sustainability and effectiveness of rehabilitation outcomes.’
Are rehabilitation services achieving value for money outcomes?
Veterans’ Affairs does not have a basis to demonstrate that its rehabilitation services represent value for money. Veterans’ Affairs has not completed market testing or established service level agreements with rehabilitation service providers to monitor and manage performance, and there is no documented rationale for selecting one provider over another when clients are referred to rehabilitation providers.
4.16 Veterans’ Affairs engagement of specialist external rehabilitation providers is a procurement process subject to value for money considerations. Value for money is a judgement on whether a procurement decision has enabled an entity to obtain services or goods that are fit for purpose, at a required quality and for a reasonable price.46 Furthermore, prudent financial accountability necessitates careful management of significant liabilities such as those under MRCA.
Increasing rehabilitation demand and expenditure
4.17 At 30 June 2015, there were 1361 open Veterans’ Affairs rehabilitation cases. Figure 4.2 shows increasing service demand as the growing number of new cases (commenced) initiated is not matched by the closure of existing cases.
Figure 4.2: Open, closed and commenced cases 2010–11 to 2014–15

Source: ANAO analysis of Veterans’ Affairs data.
4.18 Once a claim has been accepted by Veterans’ Affairs and the need for rehabilitation established, expenditure by the Australian Government for rehabilitation services is approved by Veterans’ Affairs. While departmental administration costs are capped, funding for services for clients is not budget-limited, as a special appropriation enables fluctuations in demand to be met for medical and rehabilitation services. Based on the planned costs for open cases at September 2015, the average value of an approved plan was $11 940 with 77 per cent of approved plans valued at less than $20 000. In 2014–15, the median time for a Veterans’ Affairs client to be on a rehabilitation plan was 462 days.
4.19 Overall expenditure by Veterans’ Affairs under the MRCA is growing at a fast rate, increasing the need to demonstrate value for money in rehabilitation service delivery. Table 4.1 highlights the significant year-on-year rises in expenditure for rehabilitation and related services47 as well as for incapacity payments (discussed later in this chapter) that support veterans and serving ADF members while on rehabilitation.
Table 4.1: Veterans’ Affairs’ MRCA Expenditure ($ million)
|
Services |
2011–12 |
2012–13 |
2013–14 |
2014–15 |
|
Medical |
8.5 |
15.8 |
21.8 |
25.5 |
|
Rehabilitation |
4.5 |
6.5 |
7.7 |
10.2 |
|
Other |
0.8 |
1.5 |
1.5 |
2.0 |
|
Program support |
16.5 |
19.5 |
19.8 |
17.4 |
|
Incapacity payments |
41.3 |
60.7 |
77.7 |
94.1 |
|
Total |
71.6 |
104.0 |
128.5 |
149.2 |
|
Growth on prior year total |
- |
45% |
23% |
24% |
Note 1: Program support includes MRCA and the predecessor SRCA scheme.
Source: Department of Veterans’ Affairs Budget Statements 2015-16, Appropriation Bill 1 and Special Appropriation.
Rehabilitation procurement and contract management
4.20 There are 33 rehabilitation providers contracted by Veterans’ Affairs to meet the psychosocial, case management, and vocational needs of clients. Additional medical and specialist providers and third party psychosocial rehabilitation providers may also be engaged to address requirements and priorities in particular cases under the approved rehabilitation plan.
4.21 Rehabilitation service providers are accredited by Comcare or endorsed by the Military Rehabilitation and Compensation Commission (MRCC). Service providers have not been subject to market testing, the rationale for selecting individual providers is not documented and performance is not subject to structured assessment.
Market testing of rehabilitation services and rationale for procurement
4.22 In 2012, the department commenced a tender process for rehabilitation services. The objective was to introduce greater competition amongst providers which in turn would drive down costs. However, in 2013 with the endorsement of the MRCC, the tender process was abandoned as it was unclear whether the result would deliver better value for money or provide better outcomes for clients. The department had not documented actual rehabilitation costs and pricing prior to the approach to market to assist with benchmarking of the information provided by tenderers. The department was also unclear, prior to the tender process, about their capacity to reduce fees. Such information would have enabled a clearer assessment of the value being offered. At the time of audit, Veterans’ Affairs continues to generally accept rehabilitation service providers’ fees as quoted. There is no basis to assess the competitiveness or the reasonableness of the costs or the associated time allocated for cases. It is largely determined by the professional judgement of the providers and the experience of coordinators and delegates in Veterans’ Affairs.
4.23 Furthermore, there is no documentation on the rationale for selecting one provider over another when referrals are made. This is not consistent with accepted Australian Government procurement practice and exposes the department to financial and service quality risks. The concern over the selection of providers was raised in a Veterans’ Affairs internal audit in 2010–11 but has not yet been addressed by the department.
4.24 Without any testing of the market or documented procurement rationale, Veterans’ Affairs cannot demonstrate that it has achieved value for money in the procurement of its rehabilitation services.
Performance assessment of rehabilitation providers
4.25 There are no service-level agreements with providers that reflect the focus of the Veterans’ Affairs delivery model and its emphasis on a whole-of-person approach including quality of life outcomes, rather than just return to work outcomes like most rehabilitation arrangements. Documenting the expectations of the department with delivery partners and providing feedback on performance is necessary to ensure the focus of the rehabilitation services being provided aligns with Veterans’ Affairs’ delivery model.
4.26 The ANAO is aware that there are publicly available examples that could be considered by Veterans’ Affairs for rating the performance of providers. For instance, the Department of Employment utilises a publicly accessible disability employment ‘five-star’ rating system for its service providers.48
Recommendation No.5
4.27 In order to improve the management of rehabilitation service delivery and the rationale for selecting external rehabilitation service providers, the ANAO recommends that the Department of Veterans’ Affairs:
- introduce service-level agreements for all external rehabilitation service providers that outline the expectations of the department in the delivery of rehabilitation services;
- introduce an objective performance assessment and rating scale for service providers;
- document reasons for selecting providers for rehabilitation services; and
- re-test the market for service providers once the goal attainment scaling process has been fully implemented and the department is in a position to document its existing service costs.
The Department of Veterans’ Affairs response: Agreed.
4.28 The Department of Veterans’ Affairs has agreed with this recommendation and made the following comment:
4.29 ‘All providers seeking to work with veterans are now required to demonstrate specific skills and experience in addition to the mandated Comcare requisites. These criteria will assist with the selection of providers and allow decision makers to vindicate the selection of specific providers The introduction of these requirements was a joint industry and DVA activity.
4.30 DVA is moving towards the introduction of service level agreements when engaging service providers. This solution will allow effective management of both performance and costs of providing rehabilitation services. Performance assessments for providers will be somewhat achieved by analysis of Goal Attainment Scaling data. Further measures for validating provider performance are being considered.
4.31 It is intended to consider strategic partnerships with other agencies on the collaborative opportunities for contracting providers. The maturity of the Goal Attainment Scaling implementation and data and related activities in conjunction with the next review by Defence of contract arrangements for provision of rehabilitation services will address this recommendation.’
Are incapacity payments to ADF members and veterans well managed?
Incapacity payments have not been well managed to date. In 2014, Veterans’ Affairs reported a 22 per cent critical error rate in payments, against a target of five per cent. At the time of the audit, Veterans’ Affairs advised the ANAO that it was in the process of addressing the high error rates and complaints by MRCA clients through system and process improvements, as well as considering policy adjustments.
MRCA–related rehabilitation expenditure by Veterans’ Affairs has more than doubled to $149 million over the four years to 2015 and incapacity payments to support ADF personnel and veterans represent a substantial portion of this – $94 million in expenditure in 2015.
Since inception, MRCA liabilities have grown substantially each year to $4.5 billion at 30 June 2015, of which $2.37 billion relates to incapacity payments. The growth reflects the demand-driven nature of the scheme, which is funded through an essentially unlimited special appropriation. Available performance information does not yet enable an understanding of the contribution that rehabilitation services make to the financial sustainability of MRCA.
4.32 ADF members and former members with an inability to work or reduced capacity to work because of injury or illness connected with service may access incapacity (income maintenance) payments to cover their loss of earnings. For example, if an ADF member or former member is able to work only three days per week due to illness or injury, they may be entitled to an incapacity payment to compensate them for the other two days of lost earnings. Furthermore, current ADF members with accepted MRCA liability claims are eligible for income support to make up for the loss of allowances that they would otherwise receive on deployment or in intensive training.
4.33 The MRCA rehabilitation and compensation scheme is demand-driven, funded through a special appropriation which essentially provides unlimited funding to Veterans’ Affairs for the scheme’s administration. As illustrated in Table 4.1, MRCA-related rehabilitation expenditure by Veterans’ Affairs has more than doubled to $149 million over the four years to 2015. Expenditure on incapacity payments, which provides income support to current and former ADF members undergoing rehabilitation49, has increased from $41.3 million in 2011−12 to $94.1 million in 2014–15, a 128 per cent increase. Since inception, MRCA liabilities have grown substantially each year, estimated at $4.5 billion at 30 June 2015, of which $2.37 billion (52 per cent) relates to incapacity payments. These figures illustrate the significant growth in both expenditure and estimated future liabilities attributable to MRCA incapacity payments.
4.34 Given that there is the potential for significant future growth in client numbers, as well as accumulated liabilities arising from injured and ill clients under the MRCA, effective management of overall future costs is critical.
4.35 Incapacity payments can be difficult to calculate accurately–particularly in relation to end dates for multiple allowances. At the same time as steeply increasing expenditure on incapacity payments, Veterans’ Affairs has reported the critical error rate for MRCA incapacity payments in 2013–14 at 22.1 per cent against a target of less than 5 per cent. ANAO analysis of the payments has indicated that the processing of claims involves extensive manual calculations required for each claim across multiple systems. Veterans’ Affairs advised that the department’s electronic systems are not adequate to meet the requirements of processing these claims and there is a heavy reliance on manual data manipulation, calculation and transfer of claims data. In addition, a review by Veterans’ Affairs of incapacity payments indicated that over 90 per cent of critical errors related to policy, procedures or legislation.
4.36 Veterans’ Affairs is implementing strategies to address the errors that have also been a factor in complaints against the department. A number of actions were being considered at the time of audit to reduce the high error rate for incapacity processing. These are:
- ensuring that incapacity payments more closely and objectively correlate with actual losses in earnings;
- removing the disincentive from the generous incapacity payment rates for participation in vocational rehabilitation programs and return-to-work activities; and
- improving the system for administering incapacity payments so that is simple and efficient.
4.37 The audit has identified a lack of performance measurement and reporting to demonstrate the effectiveness and value for money of MRCA rehabilitation services. Available performance information is also not able to demonstrate the contribution that MRCA rehabilitation activities have made to the overall financial sustainability of the scheme and the quality of life of veterans. Strengthening performance information would also demonstrate improved compliance with the provisions of the Public Governance Performance and Accountability Act 2013, as noted in paragraph 1.4.
Appendices
Appendix 1: Entity responses


Footnotes
1 The Safety, Rehabilitation and Compensation Act 1988 (SRCA) applied for serving ADF members prior to July 2004 and the Veterans’ Entitlements Act 1986 applied conditionally for serving members prior to July 2004. Veterans’ Affairs continues to provide support and compensation under SRCA, with an estimated liability at 30 June 2015 of $2.88 billion.
2 At the time of the audit, Defence did not have accurate, reliable and complete rehabilitation data for 2015.
3 Incapacity payments compensate ADF members and veterans for the difference between normal earnings and actual earnings when undergoing rehabilitation and/or in reduced or alternative work. The loss of allowances can be a significant factor in determining the amount of compensation.
4 Defence has advised the ANAO that this is consistent with more than a decade of high tempo overseas military operations.
5 The Safety, Rehabilitation and Compensation Act 1988 (SRCA) applied for serving ADF members prior to July 2004 and the Veterans’ Entitlements Act 1986 applied before 1988. Veterans’ Affairs continues to provide support and compensation under SRCA, with an estimated liability at 30 June 2015 of $2.88 billion.
6 Explanatory Memorandum to the Amendment Bill, available at <http://www.austlii.edu.au/au/legis/cth/ bill_em/valamb2013600/memo_0.html> <accessed 5 June 2015>.
7 Military Rehabilitation and Compensation Act 2004, s38.
8 Under the MRCA, the Chief of the Defence Force is the rehabilitation authority for serving members and the Military Rehabilitation and Compensation Commission is the rehabilitation authority for former members.
9 2013–14 is the latest full year data was available.
10 ADF Transition Handbook, 2014, available from: <http://uat.defence.gov.au/Transitions/> [accessed 23 February 2016].
11 The Defence/Veterans’ Affairs Links Steering Committee is co-chaired by the Deputy President of the Repatriation Commission (Veterans’ Affairs) and the Deputy Secretary, Defence People Group (Defence).
12 Department of Veterans’ Affairs September 2015 Stats at a Glance. Open cases are those currently active with clients receiving services. Closed cases are those where there is no current rehabilitation program being actively managed.
13 Incapacity payments compensate ADF members and veterans for the difference between normal earnings and actual earnings when undergoing rehabilitation and/or in reduced or alternative work. The loss of allowances can be a significant factor in determining the amount of compensation.
14 This includes $2.4 billion in estimated incapacity (income maintenance) liability.
15 Department of Veterans’ Affairs, Review of Military Compensation Arrangements, February 2011.
16 Department of Defence–Joint Health Command, Support for Injured or Ill Project (SIIP) – Review of current practices, Canberra, 2010.
17 ANAO Audit Report No.32, 2011–12 and ANAO Audit Report No.48, 2011–12 respectively.
18 The ANAO engaged Vista Advisory to provide audit services for the conduct of this audit.
19 The strategy was endorsed by the Secretary and the Chief of the Defence Force. Reporting on actions under the policy is considered by the Defence Workplace Health and Safety Committee, which is co-chaired by the Vice Chief of the Defence Force and the Deputy Secretary, People Strategies and Policy.
20 The DWHSC is co-chaired by the Vice Chief of the Defence Force and the Deputy Secretary People Strategies and Policy.
21 The Defence workforce comprises a population of approximately 77 000. Of this number, 57 000 are ADF members (74 per cent) and 20 000 APS (civilian) employees (26 per cent).
22 A ‘near miss’ is a new reporting category, which is designed to capture incidents that may not have involved any serious injury or illness to a member, but are noteworthy to avoid repetition in future. The redistribution of incidents across new categories can distort any comparisons over time.
23 Most referrals are made by a treating medical officer (84.4 per cent in 2013–14), with the rehabilitation assessments also triggered by a member being on sick leave or restricted duties or convalescing for greater than 28 days, or other factors such as self-referral or when a member’s Commanding Officer requests that an assessment be undertaken.
24 The Medibank contract is a non-exclusive contract that allows Defence additional flexibility to meet the diverse medical and rehabilitation needs of its personnel. Medibank Health Solutions was selected as the successful tenderer. The procurement process was not in scope for this audit and was therefore not examined by the ANAO.
25 As discussed later in this chapter, at the time of the audit Defence was unable to provide data for 2015.
26 ANAO/Comcare Better Practice Guide on Rehabilitation (2001), available from <https://www.comcare.gov.au /__data/assets/pdf_file/0020/42680/Rehabilitation_Managing_return_to_work_PUB_16_jun_04.pdf> [Accessed 4 November 2015].
27 Timely referral has benefits such as preventing long term absence from the workplace, increasing the probability of a return to work, and containing the costs of incapacity and indirect costs to Defence from lost productivity and the need for additional recruitment and training for replacement personnel. The requirement for rehabilitation to ‘occur at the earliest possible time in order to optimise outcomes’ is a requirement under Defence policy (DIG PERS 16-22).
28 The former rehabilitation case management system, HealthKeyS, was not electronically linked to the Defence incident reporting system, Sentinel.
29 See ANAO Report No. 27, 2014-15, Electronic Health Records for Defence Personnel.
30 Konekt Market Report, Vol 2 - 2015, p.15, available from <http://www.konekt.com.au/konekt-marketing-report-download/> [Accessed 4 November 2013]. The study involved 16 078 Konekt client cases.
31 The national average is calculated from survey results from injured or ill persons receiving rehabilitation rather than direct clinical data. This may result in some variance in the data.
32 Based on ADF data for the cost of recruitment and training to the base level of the categories most frequently medically separated.
33 This study follows a recommendation in the review of the MRCA in February 2011 that was agreed by the then Government.
34 Section 64, Military Rehabilitation and Compensation Act 2004.
35 The review process can be triggered earlier than 12 month if it is apparent sooner that a return to work will not be achieved and a MEC downgrade is required.
36 Being ‘held-in-abeyance’ involves holding an ADF member within Defence and is used for ADF members with a risk of immediate or imminent financial hardship following separation.
37 Soldier Recovery Centres are located in Army bases in Brisbane, Townsville and Darwin and provide centres to assist ADF members with injuries or illnesses requiring temporary or permanent detachment from their units. The Personnel Support Units in the Navy are available around Australia and have a broader range of functions and are not exclusively used for injured or ill personnel. As at August 2015, there were 850 members assigned to Personnel Support Units.
38 For injured and ill members, the ADF Rehabilitation Program provides access to Vocational and Functional Assessments and a rehabilitation consultant is expected to work closely with Member Support Coordinators and Veterans’ Affairs to achieve a smooth transition. Together these support services are designed to meet the requirements of MRCA to provide transition case management (section 64) and assisting in finding suitable civilian work (section 61(3)(c)).
39 A voluntary survey is generally conducted by Defence on a regular basis (annually).
40 ‘Whole-of-person’ means that the client’s physical, medical, psychological and social needs are intended to be taken into consideration in the planning of a rehabilitation program
41 A variety of medical and allied health professionals can also be engaged in the formulation and/or delivery of different aspects of a rehabilitation plan.
42 Quality of life outcomes are important for those veterans unable to participate in the workforce due to the extent of their illness or injury.
43 Based on the injury/illness date that is closest to the date of referral for the initial rehabilitation undertaken through Veterans’ Affairs.
44 Social Research Centre, Return to Work Survey, prepared for Safe Work Australia, July 2014.
45 Goal Attainment Scaling is a standardised scoring system to assess and report on outcomes from rehabilitation services. See Veterans’ Affairs Rehabilitation Guide, available from: http://clik.dva.gov.au/rehabilitation-library/15-goal-attainment-scaling. (Accessed 5 April 2016).
46 Department of Finance, Value for Money, Buying for the Australian Government, available from <http://www.finance.gov.au/procurement/procurement-policy-and-guidance/commonwealth-procurement-rules/cprs-value-for-money.html> [accessed 8 October 2015].
47 These expenses are not discrete and will draw on medical or other expenses required for a client.
48 The Disability Employment Services Star Ratings system measures the relative success of providers in achieving outcomes for job seekers taking part in the program based on a five point scale. Available from: https://www.employment.gov.au/disability-employment-services-star-ratings [accessed 21 October 2015].
49 Current ADF members with accepted MRCA liability claim, are eligible for income support to make up for the loss of allowances that they would otherwise receive.